Can I live without canines?
Did you appreciate the information?

Question from Yasmine, an internet user.
Hello,
I’m 18 years old and I have impacted canines, but I do not want to undergo the surgery.
So, I need your advice.
Can I live without canines?
Response
Good morning Yasmine,
I apologize for taking a few days to answer your question. You have an excellent question that is worth thinking about.
Can we live without canines?
The answer is yes, we can live without canines. Except that you are not asking the right question.
You mention having to undergo a surgery which would be done to expose and ligature the impacted canine for an orthodontic traction. Yet, you refuse the surgery. This means that your canine will stay impacted.
The right question
The right question to ask is:
What are the risks associated with keeping one or more impacted canines?
First, I will show you a few examples of occlusion without permanent canines. Then I will illustrate a few examples of damage that an impacted canine can cause.
Occlusion without canine(s)

Case #1 and case #2: canine #13 was impacted and ankylosed. Case #3: Agenesis of 2 permanent canines #13 and #23.
Cases #1 and #2 each had their canine #13 impacted and ankylosed, that is fused to the bone. It was thus impossible to proceed with their orthodontic traction. The removal of the impacted tooth was necessary. The patients were told that the removal of 3 premolars (#24, #34 and #44 for case #1 and #24, #35 and #45 for case #2) would be necessary to obtain an ideal occlusion. The Xs represent the spot where the canines would be if they existed. The first premolars #14 and #24 are identified. The replacement of canines by first premolars allows the patient to obtain an acceptable esthetic and functional result.

Ankylosed canine
The picture on the left represents the ankylosed canine of case #2. The tooth crown is delimited by the dotted line. No space was visible between the enamel and the bone, confirming the ankylosis (fusion to the bone) of the tooth. The removal was the only possible option.
Case #3 presented agenesis of the permanent upper canines (he never had them). Two premolars had to be extracted in the mandibular arch.
These cases thus show that it is possible to live without canines and have a functional occlusion.
Risks associated with an impacted canine
You must know that if you do not do anything and you keep your impacted canine, you are taking risks.
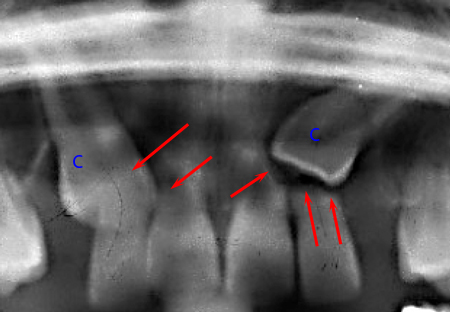
1- Formation of a cyst of the follicular envelope

Dentigerous or follicular cyst. The 13 indicates the permanent canine. The “C” indicates the primary canine. The dotted white line indicates the extent of the cyst.
A chronic apical lesion of the primary canine facilitated the development of a follicular cyst and the exaggerated movement of the permanent tooth #13.
This exaggerated upward and forward movement of the impacted canine makes the de-impaction treatment more difficult and longer.
2- Radicular resorption of permanent incisors
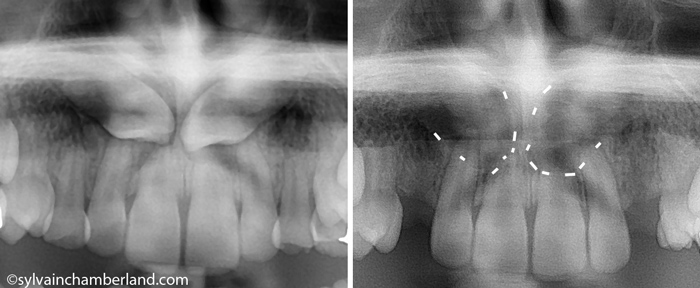
Resorption of permanent central incisors caused by two impacted canines
Incisors can suffer from resorption of their root. Note that the central incisors lost at least 50% of their length because of the impacted canines. Figuratively, we could say that there was a collision between the canine and the root of the incisor and the root “disappeared”.
In that case, we decided to extract the impacted canines, because it would have been impossible to perform the traction of these canines without causing more damage to the roots of the incisors.
Resorption of permanent lateral incisors caused by the impacted canines
This patient was lucky, because sometimes, one or more incisors need to be extracted like in this other case shown on the right.
3- Ankylosis of the impacted tooth
This problem was shown and discussed in the previous section. In such case, the removal of the ankylosed tooth is part of the solution.
Conclusion
This is just a brief summary of what can happen with an impacted canine. I did not describe every risk. It would be too long doing so.
Going back to your case, I want to understand that you do not want any surgery. But you will have to assume the risks and complications which will inevitably occur because of your decision.
Between two evils, you have to choose the lesser one. Undergoing a surgery to ligature an impacted canine is much better than any risks that you could face if you do not do anything.
You can live without canines if you do not have them, but you should not live with an impacted canine if you have any.
Think about it and make the right decision.
Hi. I’m 33. I have two deciduous upper canines ( had the adult impacted upper canines removed when I was 16 ). I would like to get a brace and wonder if they were to remove the deciduous canines and bring the pre molars forward would they need to remove teeth from my lower jaw as well ? So that my bite is still correct ?
yes this is possible in some situation, howeverI don’t know if it would be ok for you.
Both situation protracting maxillary posterior teeth or extracting 2 lower premolar could be considered. Don’t know which one would be best for you.
I had my baby upper canine teeth removed to create a gap in my teeth for my impacted canine teeth to grow down, i’ve had two springs in between my incisor and premolars for four years and the impacted canines haven’t moved a millimeter since. The ortho is now suggesting removing the impacted canines and closing the gap by bringing my premolars slightly forward and angling my incisors down since I have an overbite. I was wondering if I should get a second look by another ortho or oral surgeon. Thank you for your time.
If the canines did not move in 4 years, pronostic is not good. It maybe a good idea to extract them.
Hey Dr, i had my upper left canine removed today, as my ortho recomended, so the idea is to make the first premolar the new canine, so, i wanted to now, will it look weird? I tried to look online for pics of cases like mine but I just couldn’t find it, thanks.
What will happen on the right side?
What will happen to you maxillary dental midline?
It is not a big problem to have a premolar in position of a canine. I do have this in my mouth. The important point is to have the midline of the teeth align with the facial midline.
Hi, i did a panoramic x-ray because of the pain i felt for so long and the result was bad. I got 4 impacted wisdom teeth and 1 impacted canine. I would like to ask for your opinion, if it’s ok not to remove my impacted canine under my lower right side of the teeth? The tooth can be felt by my tongue, it really is at the side of my tongue and im kind of afraid of removing it.
Your situation need carefull evaluation. One of them, is it feasible to bring your canine into the arch?
Is it deeply impacted? If you can feel it with your tongue, it may not be that deep.
I can’t give you a good advice without seeing the panogram and doing a clinical exam.
Hello Dr I had my one of my canine’s removed on my left side when I was 11 and I got braces when I was 15 and I have a gap between my lateral incisor and my first premolar. Now a year later my orthodontist finally put a spring between the second premolar and the first premolar to try to push the first premolar to the lateral incisor. But I’m wondering won’t that just make a space between the molars and if so will they push those together and therefore have to push all the teeth on my upper jaw to the right to close the gap. I’ve had these braces for a year how much longer do you think I’m going to have them on for. Do you think I’d be likely to get them off in the next 6 months
The key question would be if the upper dental midline is coincident to the facial midline.
Yes you may need protraction of all posterior teeth on that side and it may take more than 6 months.
Hi Dr Chamberland, you’ve got some incredible advice here! I’m a 33 yo male with one horizontally impacted canine as seen in the pic. I have been feeling guilty that I chose not to get it pulled down when I got braces when I was 20. Could you please look at it and see if it is actually in a favorable location to have been pulled down? Based on what I’ve read, it is probably not, because the angle to midline is 60 or more and it is at the top third of the adjacent incisor, possibly risking damage to the latter’s root upon pulling. I still have the deciduous canine and I have no symptoms. My ortho said the latter looks strong and may last me a lifetime. What do you think is the best management in this situation? Leave it alone or do something? Thank you.
https://photos.app.goo.gl/ndTopLE17LtgRKM57
I was told by my ortho that it is a difficult case esp at my current age, because of the horizontal aspect of the impacted canine and the proximity to the roots. If done, how long do you expect this to take to get the canine into position?
Bringing an impacted canine into occlusion takes time. It is not a reason to not try. Rome was not built in one day.
It will be worth the effort to get your canine in occlusion.
I would generally prefer to avoid orthodontic treatment at this time as I work full time in a very demanding job. I may not be able to make regular appointments for adjustments. What would you recommend other than orthodontic treatment?
If you can’t do orthodontic treatment and want to do something that will favour canine erution, You MUST remove the primary canine ASAP.
Hello, I have a class 2 division 2 malocclusion and a palatially impacted maxillary canine. My ortho said that as I am 34 it would be very difficult to bring down the impacted tooth with orthodontics so I had it removed. He is going to align the teeth and has given me two options to disguise the malocclusion. Option 1: extract one upper pre molar & one deciduous canine (which I still have at 34 years old!) and move all teeth back or Option 2:remove both upper premolars and replace deciduous canine with implant. Any advice you could give me would be gratefully received.
I would, by far, recommend option 1: extract 1 upper premolar and the deciduous canine on the other side. I had a canine removed in my early teens and I spent all my life with a 1st premolar on one side and a canine the other side.
I would NOT extract a good premolar and then later place an implant to replace the missing tooth.
I’ve permanent canine teeth inside my upper jaw. Doctors said they have to be removed because of which I got a gap.between my two incisors. Today I went to the hospital and doctor tried to remove the tooth but he couldn’t as they are difficult to extract.. he somehow extracted two pieces of one canine but not completely. The procedure was so painful. Now I don’t want to continue with that. I just want to kmow that whether me of nor continuing with the further surgery make any complications?
I would like to know if it was an oral surgeon who tried the extraction. It is very unusual.
My 11-year old daughter has just been diagnosed with “class II division malocclusion on a mild skeletal II base complicated by (1) diminutive UL2 and UR2; (2) Impacted UL3 and UR3 with possible cystic change and associated root resorption; (3) retained EDC/CDE (both upper/lower); and (4) upper arch crowding.
We are awaiting further test (on cystic change/root resorption) but initial recommended treatment is to either remove the two diminutive incisors (and shape the canine to look like incisors) or to remove the two canines.
Reading your article has reassured me that removing the canines can be the right choice (I had previously only come across removal of premolars in orthodontic treatment) but I’d really welcome your thoughts on these options. In particular the two concerns I have are: with the first option wouldn’t the ‘shaping as incisors’ risk compromising the robustness of the teeth? And wouldn’t either of these approach risk leaving gaps between the incisor/canine group and the molar/premolar group (I understand it can be difficult to move molars/premolars forward).
Bonsoir,
If the lateral incisors are smaller than normal and in a peg shape, it could be a good choice to revome the lateral incisors and do the substition with the canine when a patient has a class II relationship.It is feasible to make the substition without leaving gap. Particularly if the patient is class II.
However, your orthodontist should discuss with you the possibility of regain a class I molar relationship and not proceed to extraction.
It is very unlikely that I would plan extraction of the permanent canine in a 11 years old patient.
My final recommendation is to remove the deciduous canine and reassess after 6 months. Often time, maxillary expansion AND extraction of deciduous canine is effective in interception of impacted canine. I would delay as much as possible the extraction of any permanent teeth.
Hi, my daughter is 12 yrs and previously she had her upper premolars extracted to pave way for the canines which were stuck in. Then yesterday when she was being extracted the lower premolars to balance the top, one of the canine was extracted by mistake and her dentist advised to remove the other canine to balance instead of the premolars. Now my daughter has upper canines and no lower canines will it have any negative impact on her?
Oupps!
This is a major mistake. I would not fix a mistake by doing a 2nd mistake. Personnaly, I would manage mechanics, keep the other canine and extract the 1st premolar. Did you take action against the dentist who extract the wrong tooth?
Having said that, it could be a good solution to extract the other canine, but chances that I would not do that.
I have an impacted canine upper front jaw. I also have braces, my oral surgeon stated I should get the impacted canine remove, once my ortho start moving teeth, my front won’t get damage and possibly losing them. So I had the surgery done two days ago, my surgeon only remove half of my impacted canine. The other half won’t move. The surgeon kept pulling but it won’t move. So he decided to leave the half in.
He said I should be fine, the piece he remove was near my front teeth. I should be fine when my ortho start moving teeth.
My question is it safe to leave half of an impacted canine in????
If a part of the root is left in place, I hope it will not jeopardize the root of adjacnet teeth as they are moved to close the space of the extracted canine.
There is situation where it is indicated to partial odontectomy like in the removal of an impacted 3rd molar.
I would recommend that your dentist or orthodontist follow up with panogram in 6 and 12 months to make sure it remain safe.
I have one question. How the orthodontist the asymmetry that is created by the extraction of 1 tooth?
If canines are burried in the palate and if the patient refuses the treatmet, what is the patient supposed to expect in the future regarding his/her teeth and faciual struture
I think this page is very clear on the risk associated with impacted canines: follicular cyst, root resorption of the adjacents teeth which will lead to tooth loss.
A parents that would refuse the treatment of an impacted canine of his child will have to live with the full responsibility of damage that may occur in the development of the dentition.
Like I said:
You can live without canines if you do not have them, but you should not live with an impacted canine if you have any.
The risk of developing pathological conditions as a result of retention of an impacted tooth is low, with the exception of decay/resorption of the roots of adjacent teeth. It is often said that an impacted tooth may be asymptomatic, but that does not mean that they will remain that way!
As an Oral and Maxillofacial Surgeon who routinely removes impacted teeth, I do suggest removal of impacted cuspids. Tiis advice is always tempered with a recognition of the risks that may be associated with the removal of the tooth/teeth. Impacted cuspids can be some of the most difficult teeth to remove and can give riise to issues such as oro-nasal or oro-antral fistula. Surgical exposure and application of orthodontic traction is not always an option and will depend on the location of the tooth in the alveolar bone. It is always best to discuss all risks, complications and benefits with an Oral and Maxillofacial Surgeon before making a final decision over management of an impacted tooth, cuspid or otherwise.
Thank dr McCann
I think case #2 “radicular resorption of permanent incisors” and case #3 “ankylosed canine” are exemple where surgical exposure and traction is NOT an option.
Best regards
Excellent description of the choices in your example cases and the problems of NOT identifying and correcting impactions. The correct final statement!
Pat Ohlenforst
Irving, TX
Thank you Dr Ohlenforst for your comments.