Can lower jaw growth be stimulated?
Question :
Hello, my 5-year-old son’s dentist advises me to consult an orthodontist because according to her, he has a Class II malocclusion (very small chin). She believes that his chin has stopped growing after he got hit on the jaw.
When he closes his mouth, molars on molars, we can see his upper deciduous teeth covering completely his lower teeth. They are straight although we can see a small gap between his upper incisors.
On different orthodontists’ websites, they suggest to only work on the problem at around 11-15 years of age when children are in full growth. On others (European), they say to work on it as soon as possible to stimulate jaw growth. It is hard to know what to do when information is contradictory.
I would obviously like to stimulate the growth of his chin. Is there something to do in that sense? Thank you for giving me your advice.
Réponse :
Miss Di Cesare,
Your question includes 2 parts that I will summarize as follows:
1- Can a chin stop growing following a hit on the lower jaw?
My answer will be according to the following interpretation: Can a hit, an impact on the lower jaw, affect the forward growth of this jaw?
2- Can an early treatment (7-10 years of age) in 2 phases (1 phase with a functional appliance (Bionator, Frankell, orthopaedic devices) followed by a second phase with fixed appliances) can stimulate lower jaw growth and be beneficial compared to a similar treatment performed later in only one phase (12-14 years of age)?
1- Hit on the lower jaw
A single hit on the jaw will have little effect on mandibular growth and your son’s Class II malocclusion can be explained in a totally different way than an impact. The apple never falling very far away from the tree that bore it, heredity (from the father or mother) is the explanation that must come first. Indeed, physical characteristics of an individual are hereditary and a malocclusion, whether it be Class II or Class III, is a physical characteristic, so, consequently, hereditary.
With that being said, a young child can hit his chin when falling and fracture one or both mandibular condyles. This will have an effect on the forthcoming mandibular growth. For more details, consult the page Child with hypoplasia of the processus condylaris and caput mandibulae on the left.
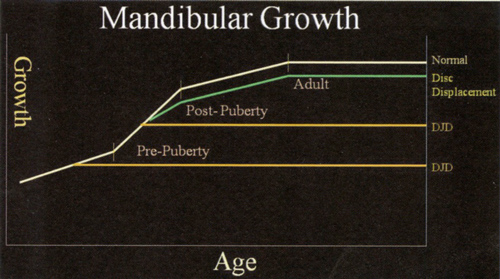 If there are no fractures, contusion (compression) could cause damages to the articular surface. If the effect of a fracture can be seen quite quickly after the event (impact), the effect of contusion can be seen later. The figure on the opposite side shows a slower mandibular growth curve (green line) than normal growth which occurs in the absence of trauma and internal derangement.
If there are no fractures, contusion (compression) could cause damages to the articular surface. If the effect of a fracture can be seen quite quickly after the event (impact), the effect of contusion can be seen later. The figure on the opposite side shows a slower mandibular growth curve (green line) than normal growth which occurs in the absence of trauma and internal derangement.
I point out that I do not believe that it is your son’s case.
2- Early treatment in 2 phases versus late treatment in 1 single phase
In the 1990s, 2 major research projects using a randomized clinical trial method were conducted by the University of North Carolina (Dr Camila Tulloch and Dr William R Proffit) and by the University of Florida (Dr Greg King and Dr Tim Wheeler). More recently, an important similar research project was conducted at the University Manchester in the United Kingdom (Dr Kevin O’Brian and Dr. J. Wright).
These projects provide us with the best data available to understand the response obtained by treatment of growth modification in Class II malocclusions. The trial conducted at UNC on a 10-year period compared 2 treatment strategies.
1- Treatment in 2 phases: an early treatment in mixed dentition, before adolescence, followed by a second phase of treatment in permanent dentition.
2- Treatment in 1 phase: a treatment during full growth of adolescence at the beginning of permanent dentition.
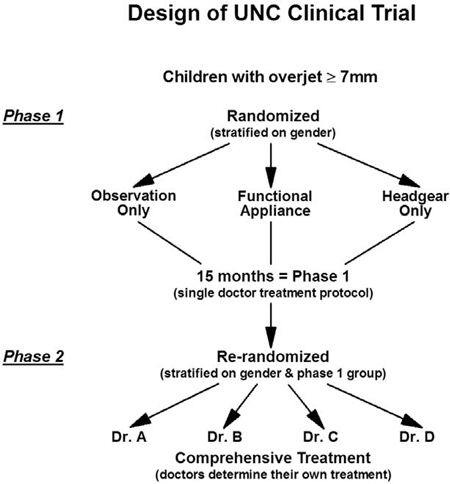 During phase 1, patients were assigned randomly (randomization) either in an observation-only group (no treatment), either in a group with treatment using a functional appliance (bionator), either in a group with treatment using a headgear. They were followed for 15 months.
During phase 1, patients were assigned randomly (randomization) either in an observation-only group (no treatment), either in a group with treatment using a functional appliance (bionator), either in a group with treatment using a headgear. They were followed for 15 months.
During phase 2, all patients were reassigned randomly to 4 treating orthodontists. Those who were in the control group and whom had not received any treatment started theirs.
Groups who had received a treatment were compared to the group who had not received any at the end of phase 1.
At the end of phase 2, the research project emphasized on the comparison of results of those who had already received an early treatment to those who had not received any treatment in phase 1 and who were treated only during adolescence.
.
Results of a 2-phase treatment versus a 1-phase treatment
Data from these research projects make it possible to conclude that:
1- In average, a child treated with a headgear or a functional appliance before adolescence will obtain a small but significant correction of the Class II intermaxillary relationship compared to a control group of untreated children. About 75% of treated children before their puberty growth had a favorable response.
2- Change in the skeletal relationship obtained during the early treatment phase is partially lost and is not maintained during subsequent mandibular growth, whether it be for the headgear group or the bionator group. Indeed, an early treatment has little or no effect on subsequent skeletal changes, alignment of teeth, occlusion, duration or complexity of treatment.
3- At the end of the major treatment (phase 2) performed during adolescence, there are no differences between patients having received a phase 1 and those who had not. This means that a 2-phase treatment initiated before adolescence in mixed dentition is not more efficient than a treatment initiated during adolescence in permanent dentition. An early treatment is thus not efficient since it does not shorten the duration of treatment with fixed appliances during phase 2, does not decrease the complexity of such phase 2 treatment whether it be in terms of extractions or orthognathic surgery.

The figure on the opposite side shows the effect of a “so called” acceleration of growth during the phase of treatment with functional appliance and return to normal once the use of functional appliance is stopped. This shows that there was no “stimulation” of mandibular growth, but only acceleration, because if stimulation had occurred, the growth curve would not have returned towards a normal growth curve.
Conclusion
Consult an orthodontist when your child will be 7 years old. Do not rely on European sites concerning early treatments, they are a little behind on this kind of news…
It is not impossible that your child could benefit from some interceptive treatment, but it is not likely that it could be beneficial to receive a treatment to stimulate growth of his jaw before he is 12-13 years old (depending on his physical maturity level at that moment).
The systematic review (meta-analysis) of Drs J.E. Harrison, K.D. O’brien and H.V. Worthington, Orthodontic treatment for prominent upper front teeth in children, published in 2008 in the Cochrane database concludes that:
The evidence suggests that providing orthodontic treatment, for children with prominent upper front teeth, in two stages does not have any advantages over providing treatment in one stage, when the children are in early adolescence.
References:
Harrison JE, O’Brien KD, Worthington HV. Orthodontic treatment for prominent upper front teeth in children. Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD003452. DOI: 10.1002/14651858.CD003452.pub2.
Gregory J. King, et al, Comparison of peer assessment ratings (PAR) from 1-phase and 2-phase treatment protocols for Class II malocclusions, AJODO 2003;123:489-96.
Proffit WR, and Tulloch J. Preadolescent Class II problems: Treat now or wait? American Journal of Orthodontics and Dentofacial Orthopedics. 2002, Jun;121(6):560-562.
Tulloch JF, Proffit WR, and Phillips C. Outcomes in a 2-phase randomized clinical trial of early Class II treatment. Am J Orthod Dentofacial Orthop. 2004, Jun;125(6):657-67.
Tulloch JF, Proffit WR, and Phillips C. Influences on the outcome of early treatment for Class II malocclusion. Am J Orthod Dentofacial Orthop. 1997, May;111(5):533-42.
Tulloch JF, Phillips C, and Proffit WR. Benefit of early Class II treatment: progress report of a two-phase randomized clinical trial. Am J Orthod Dentofacial Orthop. 1998, Jan;113(1):62-72, quiz 73-4.
This information on your website regarding stimulating lower jaw growth in adolescents is very interesting to me. My daughter will be 14 in December. She is missing half of her permanent teeth. She has reduced upper and lower jaw growth. We have consulted several specialists over the past years including a maxillofacial specialist who states she could have lower jaw surgery sometime after the age of 16. I want to make sure we are doing everything we can to stimulate jaw growth while she is younger. One orthodontist mentioned placing braces that will then cause ‘mini’ breaks in the jaw that encourage bone growth. I am a Speech Pathologist and work with patients on feeding and speech exercise including jaw strength and other areas and am curious if chewing exercises can stimulate more growth (see also Diane Bahr, SLP or Sara Rosenfeld-Johnson, SLP websites and info.). I have read articles regarding stimulating jaw growth with devices such as a Crozat, MARA, Herbst, headgear, etc. Any advice is greatly appreciated!
Keep in mind that there is no appliances, muscles exercices, speech exercises, chewing exercices that can grow mandible. This is pure quackery and snake oil.
I would follow the recommendation of your maxillofacial specialist.
My 7 years old son was seen by two orthodontics, said he needs the phase 1 treatment immediately to stimulate his lower jaw to grow and the other said we should wait at leas one or two years I really don’t know what to do
I would not recommend treatment to make the lower jaw grow at such a young age because research have shown that there no appliance that can make the lower jaw grow more than what is inherited.
I assume that your son has a class II malocclusion. You chould wait until age 11-12 and get a comprehensive orthodontic treatment at that moment.
Hope that help.
Best regards
Thank you ver much for your reply dr Sylvan. I think I am going to wait as you recommended ting is his one of His permanent lower tooth (22) is growin behind the other one due to space that is what worries me woul Orthp would be able to fix that?
You should consult an orthodontist for the crowding and the class II. There might be something to do that would help resolve the crowding. It may be serial extraction or rapid maxillary expansion and it can be done at 7 years old.
From the article I understand that an early treatment has little or no effect on subsequent skeletal changes, alignment of teeth, occlusion, duration or complexity of treatment, in comparison with starting during adolescence (phase 2). In one of your comments you write: research have shown that there no appliance that can make the lower jaw grow more than what is inherited. Do you mean that even if you would wear an activator appliance during adolescence, that it would not stimulate growth but only accelerate it achieving the same skeletal end result (adult mandible size)?
Yes. There is no functional appliance that can make lower jaw grow more than inherited.
A functional appliance move teeth on the bone but not grow bone.