Child with hypoplasia of the processus condylaris and caput mandibulae on the left
Question :
Fracture condylienne, hypoplasie du condyle mandibulaire et asymétrie faciale
Condylar fracture, hypoplasia of the mandibular condyle and facial asymmetry
Dear Dr Sylvain Chamberland,
My name is N. P. and I am a medical oncologist from Russia.
My friend from Boehringer Ingelheim who is collaborating with Prof.
Eikelboom recommended you as a great specialist on the problem.
I was wondering if I could request you kindly to provide a
consultation for a 7 year old girl with hypoplasia of the processus
condylaris and caput mandibulae on the left via internet. I could
provide all the relevant information on this clinical case including
CT and photos.
I am very sorry for the inconvenience but we have different treatment
recommendations from various specialists and we have doubts about the
diagnosis and pathogenesis of this condition. We really need the
second and independent opinion.
We would very much appreciate if you could help us.
Here is the case:
The 7 year old girl has been glowing and developing normally. She had no birth trauma. Please see the photo 01.
The child had regular dentist checkups twice a year and no pathology was revealed.

For the first time the dentist payed attention to the deviation of the lower jaw to the left when mouth opening in May 2013. The child was examined by orthodontist at the same day and it was evaluated as functional disorder. The centrum of upper and lower teeth was not displaced. It was recommended to follow up the child for a year.
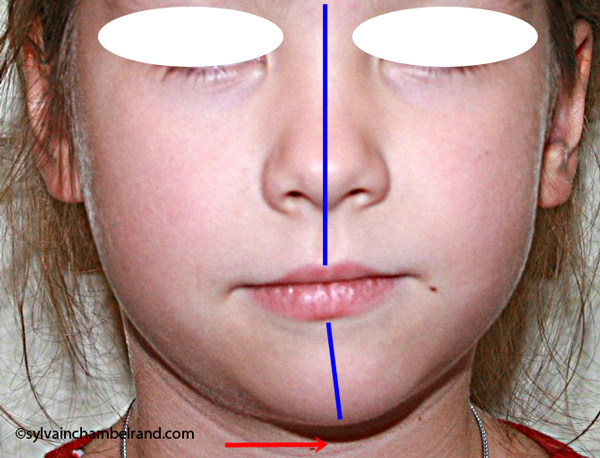
This summer the child has grown up rapidly and parents noticed asymmetry of the face when the head was lifted up. Please see the photo 02.
The child does not have any complaints. She can open the mouth wide enough and there is no discomfort in the left temporo-mandibular joint at all. Please see the photo 03 and 04.
Hearing is not impaired. Both ears are well developed.
According to ECHO the child also has signs of connective tissue dysplasia – myxomatous changes of mitral valve leaflets with mitral valve prolapse; mitral, tricuspid and pulmonary valves insufficiency (grade 1). Earlier planovalgus deformity was diagnosed, it was successfully corrected to normal. Dysplasia of coxofemoral joints was excluded (X ray). Other signs of connective tissue dysplasia are unknown.

The child was examined with computer tomography (the link to CT images will be sent in the next e-mail), teleroentgenography in the lateral view (reconstructed from CT – please see the attachment “TRG”), ortopantomografia (reconstructed from CT – please see attachment “Panoramic”) and detalization of the left temporo-mandibular joint (reconstructed from CT – please see attachment “Joint”).
After questioning the child remembered that 2-3 years ago she had hit her chin with the metal crossbar ladder. The impact was strong enough. But the parents cannot confirm this.
The diagnosis varies from congenital to acquired and treatment recommendation – from conservative orthodontic and surgical at the age of 14 to distraction osteosynthesis now and orthodontic management afterwards with repeated surgery if wanted.
We would very much appreciate your consultation and we are very sorry for the delay.
—
Kind regards,
Dr N. P., MD, PhD
Biotherapy Department
N.N. Blokhin Russian Cancer Research Center
Moscow, Russian Federation
Réponse :
Dear Dr P.,
I want to thank you for you question as it permits me to address an underestimated cause of facial asymmetry in young growing children.
I commend you for the quality of the case analysis and the quality of the picture you sent me.

The most likely diagnosis for the facial asymmetry of this young girl is an undiagnosed condylar fracture that most likely happen when she falled on a metal crossbar bar ladder 2 or 3 years ago while she was 4 – 5 years old or so. The condylar stump has healed and a new condylar head has formed, but the losted substance of the condyle is gone. Therfore, the height of the ramus has shortened.
On the xray picture, # 1 indicates the right condylar head, #2 the right articular eminence, #3 the left articular eminence and #4 the left condylar head. It is obvious that the left ramus and condylar neck are shorter and the left eminence has no slope if any. Healing and normal growth had reshaped both condyle and eminence.

When looking to the condyle from an anterior view, one can see the familiar oblong shape of a condyle but the left condyle is smaller.
You mentionned that beside a deviation to the left when opening (see above pict) there is no limitiation of the amplitude (it is obvious when looking at the picture) and there is no discomfort for the patient.
This remind me the caveat of Dr Bill Proffit: “If it can move, it can grow. If it don’t move, it will not grow.”
This young girl was fortunate to not experienced any limitation of jaw opening movement and prolonged discomfort, except when the accident has occured.

There is one minor thing I disagree with your diagnosis. The midline are not coincident. I traced the upper and lower midline on the right picture. Note that the lower midline is toward right like the occlusal plane canting to the right. This can be explained by the lack of heigh of the left ramus and as normal growth occur, there is a wagon wheel effect and the midline deviate toward the normal side, the occlusal plane is moving up on the affected side.
What should we do now?
It is sad that such event occur in children.
I think the best attitude would be to wait and see. Monitor her dental and facial development until age 13-14.
Chances are that she will have a class II molar relationship in the left side and a class I (may be a class III) molar relationship in the right side.
A decision will have to be made regarding her occlusion and her facial asymmetry.
Treatment may involve an asymmetric extraction pattern (no extraction in the lower left quadrant). It is hard to tell so long time in advance.
Chances are that an orthognathic surgery might be indicated if this pretty young girl wish to have a symmetric face during adulthood. But chances are also that she might be ok with some asymmetry.
I am aware of one publication of Dr Birte Melsen who reports 3 cases where hybrid functional appliance was used to correct the asymmetry. In this case, if i would have to try something, I would use an hybrid of bionator in the right side and Frankell II in the left side. The goal would be to disctract the left condyle from the fossa, create an open bite in the left side to allow vertical dentoalveolar growth while restricting to some extent the dentoalveolar growth with the bite plane in the left side. I would not garanty if it would work, but it is the only think I can think of at this age if the parents insist of doing something
I would not recommend osseous disctraction at this age neither would I recommend it at the adolescence. The fibrocartilage of the condylar surface has been damage and she is lucky to have a regenerated condyle even if it is smaller. Doing osseous disctraction would generate significant pressure on the newly formed fibrocartilage and resorption is likely to occur. This would be drammatic. I would prefer an hybrid Bionator-Frankell rather than osseous distraction.
Conventional orthodontic treatment and, if necessary, an orthognatic surgery, are much more predictable than osseous distraction of a ramus with a reshape fractured condyle.
Finally, I want to share with the case of a 5 years 10 months girl who falled on her chin and suffer bilateral condylar fracture. It was in september 2006. Please look at the panoramic radiograph and note that both condylar head are displaced anteriorly. The right side seem more damaged thant the left side.


Seven year later she was ready for the orthodontic treatment. Note her facial asymmetry to the right, cant of the occlusal plane to the left, deviation of the lower midline toward the side that is longer vertically. Orthodontic treatment is going well. I delayed the orthodontic treatment as much as I could.
The radiograph taken in july 2013 show a small reshaped condyle in the right side while the left condyle has a more normal form despite its previous fracture.
I wish all those information will help.
Note that the analysis of the case you submitted is only an opinion on the data you sent and should be interpreted with caution because i did not do a clinical exam.

For more information on facial asymmetry, I recommend this Keynote: Hemimandibular Hyperplasia and Facial Asymmetry.
Slide from 89 to 98 describe talks about condylar fracture.
Bibliography
Proffit WR, Vig KW, and Turvey TA. Early fracture of the mandibular condyles: frequently an unsuspected cause of growth disturbances. Am J Orthod. 1980, Jul;78(1):1-24.
Melsen B, Bjerregaard J, Bundgaard M. The effect of treatment with functional appliance on a pathologic growth pattern of the condyle. AJODO. 1986;90503-512.
I am a 53 year old woman who has TMJ. Found out back in 1990, when working for an orthodontist at the time, wanted to test out a new panoramic X-ray machine. To my surprise he told me that my mandible was broke off at the condyle! I can’t remember when this happened. He suggest going to Dr Pamela Stead in Indianapolis. She had taken more xrays, photos showing my misaligned jaw and dental molds of my teeth ( which my back molars on the side of my jaw problem are lower than the other side). Dr Stead started treating me with an appliance to help with the TMJ and neck pain. Over the years I notice that my smile is crooked and my face also. I absolutely hate it! Wished that I knew when this happened as a child and that someone could of helped with the alignment of my bite and off center of my smile!
It is not to late to fix you crooked smile. You may require orthognatic surgery to correct your occlusion (and face) in the 3 planes of space.
My name is Arghavan and I am a general physician in I.R.Iran.
I have had the same problem that this little girl has, I had a neglected condylar fx when I was 1 year old ,
The diagnosis was confirmed 2 year later when my parents began to notice the asymmetry in my face.
The doctor said I should wait until I’m 21 so I did.
2 years ago when l was 25 I finally got a correction surgery which unfortunately did so little for my problem. If you are interested I can email you my profile and my CT scan before and after the surgery. I hope to find a way so my face can become fully symmetric because it has impacted my self esteem a great deal.
Regards
You can send your photo and CT scan to my professional facebook account: facebook.com/drsylvainchamberland. If you do so, it means that you authorize me to publish it. Of course I will hide your identity and block your eyes to make sure your anonymat is preserved.
I will change your identification and use only your 1st name.
Bonspir Tushar,
I moved your question to this page where it is more suitable with the topic of the page.
I think you should consult an orthodontist and an oral surgeon as soon as you can. At 16 years old, you are near the end of your adolescent growth period. Chances are that you will need orthodontic treatment along prior to maxillofacial surgery.
It is normal that your face became more and more asymmetric from 13 to 16 as you had normal growth on the right side while the left side had impaired growth.
Did you had reduce mobility in term of jaw opening? I wish not. Decrease mobility is a sign of ankylosed joint.
I show you a panogram of an adolescent who had bilateral condylar fracture, fracture of the left maxilla and fracture of the mandible on the right side at 14 years old.She was having an ortho treatment. The oral surgeon call my office to have the photo of the patient to put the pieces together…
She had reduction of the fracture of the left joint only. The growth of the left joint was significantly reduce, but the right joint resume to normal growth with no sequela. The consequence is that she have some faical asymmetry to the left. A bimaxillary surgery was necessary.
This is the panogram post accident
The second panogram show the result after a bimaxillary surgical phase that was necessary to correct the assymmetric facial growth that occur some 5 years after the car accident. One can see the normal growth of the right condyle, but impaired growth of the left condyle.
hello,
i am a boy age 16 i had an accident at the age of 13 due to which my left jaw joint was fractured .
when i see my face in the mirror i see that my right size is growing normal whereas my left isnt growing ,,
my face is getting assymetric and i am really worried .
i want to know how can i treat it and at which age should i start the treatment
You did a nice job in your discussion, but it appears that she has reasonably good opening, and I think trying a hybrid functional appliance now would be a good idea. She isn’t going to get better without treatment. I illustrated a somewhat similar patient in the 4th and 5th editions of ContemOrthod, in which there was a positive response to hybrid functional treatment.
Thank you Dr Proffit,
Your input is very much appreciated. In the AJODO 1980′s article, there is a picture of an « Hemi-Frankell » and I do remember having see a similar patient in an edition of Contemprary Orthodontics.
Happy Thanks Giving
Best regards
Sylvain