Surgical technique
Did you appreciate the information?

Surgical exposure techniques may vary depending on the location of the impacted canine, whether it is on the palatal side or the buccal side.
Two authors, Dr Vincent G. Kokich from the University of Washington in Seattle and Dr Robert L. Vanarsdall from the University of Pennsylvania in Philadelphia have greatly published on surgical exposure techniques of impacted canines. They are two world famous leaders on the matter.
Dr Kokich recommends open and preorthodontic exposure of palatally impacted canines. This facilitates eruption and orthodontic traction.
Dr Vanarsdall recommends open exposure with a repositioned gingival flap (pediculated connective tissue graft) above the impacted canine. This allows a better gingival architecture around the canine once the orthodontic treatment is finished.
Surgical techniques are thus divided into 2 main categories:
• Open exposure and eruption (open eruption technique)
• Closed exposure and eruption
Historically, in the Quebec City area, the closed exposure and eruption approach has been more often used. Orthodontists from Quebec City are lucky to be able to rely on an excellent group of specialists in oral and maxillofacial surgery and they have great ability in manipulating soft tissues and they bond the cleat to the tooth and put in place the metal ligature wire.
Open exposure and eruption
Palatally impacted canine

Kokich surgical technique for impacted canine
• The palatal flap must have the right size.
• Meticulous ostectomy of the bone covering the canine crown must be performed.
• The soft tissues (follicular envelope surrounding the permanent tooth crown) must be removed down to the cementoenamel junction.
• Reposition the flap in its former place and make an opening in the flap to expose the crown and the bonded cleat.
• Put a periodontal pack (dressing). This allows healing without having the tissue cover the tooth again during healing.
• Wait 6 to 9 months before initiating orthodontic therapy.
Kokich VG. Surgical and orthodontic management of impacted maxillary canines. Am J Orthod Dentofacial Orthop 2004;126:278-283.
Kokich VG. Preorthodontic Uncovering and Autonomous Eruption of Palatally Impacted Maxillary Canines, Semin Orthod 2010; 16: 205-211
Transmucosal open exposure of impacted canines
A colleague from Ontario provided me with a few examples of canine exposure. Notice the eruption of canines within 7 months. However, due to the severe lack of space (no space available between the lateral incisor and the premolar), the following is a legitimate question to ask: Wouldn’t it have been preferable to extract both first premolars and thus offer the canines space that would have allowed eruption in the arch rather than in the middle of the palate?
Surgical technique to expose palatally impacted canine
The current series of pictures show the exposure technique as it is generally performed by oral surgeons from Quebec City.

Surgical exposure technique and ligation of a palatally impacted canine. Oral surgeon: Dr Michel Fortin
• The full-thickness palatal flap (including the periosteum) is wide, spreading from the papilla anteriorly to the second premolar posteriorly. The vasculo-nervous bundle of the nasopalatine duct (under the nasopalatine papilla) is preserved.
• An ostectomy allows the exposure of the crown of the canines.
• The follicular envelope is removed down to the cementoenamel junction. No remnants of the follicular envelope must be left in place, because it could prevent bone healing and reattachment of the ligament to the tooth.
• Cleats are bonded to the exposed and most accessible surface of the tooth. On the right, the cleat was bonded to the lingual surface. On the left, the cleat was bonded to the buccal surface. To distinguish right from left, you have to know that you look at the patient in front of you, which means that his right is on your left.

Closed palatal flap and orthodontic ligation. Oral surgeon: Dr Michel Fortin
• The palatal flap is closed and sutured in place with absorbable thread (sutures).
• An opening is made in the flap to allow the metal ligature wire to pass (twisted 0.01 orthodontic ligature wire). The opening in the flap on the left side of the image is not wide enough. During healing, the remaining palatal tissue will cover the canine too much and will slow down its eruption (see following page entitled Mechanotherapy).
• The ligature wire is bonded to the cleat.
• The ligature wire surrounds the orthodontic arch until the orthodontic traction is activated.
• At this stage, a periodontal pack could or should be placed to prevent the covering of the transmucosal openings during healing (healing by second intention).
• Orthodontic traction is initiated 7 to 10 days after the surgery.
Note that since the anchor point is different on canines, we have to expect that the right canine will rotate and that its lingual surface will be visible first due to the fact that the cleat is bonded to the lingual surface. For the left canine, the buccal surface should erupt first since the cleat is bonded to the buccal surface.
Surgical exposure technique on an impacted canine in vestibular position

Impacted canine in vestibular position
When the canine is located on the vestibular side (black circle), it is recommended to use an apically repositioned flap to bring an adequate band of keratinized gingiva to the neck of the tooth.
Keratinized gingiva is pinkish and attached more firmly to the subjacent bone than the alveolar mucosa. The black arrows indicate the line of the mucogingival junction between the mucosa and the gingiva. The keratinized gingiva under this line must be above the erupting tooth. Usually, the tooth breaks through the gingiva at the crest of the ridge and keratinized gingiva will cover the neck of the tooth.
The surgical exposure of the case of the canine on the opposite side is illustrated in the series of pictures below.

Apically repositioned flap for open eruption technique of an impacted canine. Oral surgeon: Dr Jean-Philipe Fréchette.
• The initial incision is made at the crest of the ridge. Two loosening vertical counter-incisions go back up to the oral vestibule. The gingival flap is dissected from the periosteum which stays in place. We say that it is a half-thickness flap because it does not contain the periosteum. The periosteum is that nutritious membrane covering the bone and composed of bone-forming cells.
• An ostectomy (removal of layer of bone) allows exposure of the canine crown.
• A cleat is bonded to the surface of the tooth and a metal ligature wire is fixed around the head of the cleat.
• The keratinized gingiva which was located at the crest of the ridge (black rectangle on the left) is apically moved (green arrow) to the top of the bone opening (black rectangle on the right).
• The flap is sutured in place.
• The exposed periosteum changes into granulation tissue and allows healing by second intention. Healing by second intention means that the wound closes by proliferation of healing tissues around the wound. Healing by first intention occurs when the wound edges can touch and reseal. A skin incision that necessitates stitches to reseal the wound is an example of healing by first intention.
Vanarsdall RL. Efficient Management of Unerupted Teeth: A Time-tested treatment modality, Semin Orthod 2010;16:212-221
Vanarsdall RL, Soft-tissue management of labially positioned unerupted teeth, AJODO 2004; 125:284-293

Healing after 12 days of an apically repositioned flap
Healing takes place quickly and with very little pain. The young patient told us that she had had more problems with her pain medications which contained codeine than with the exposed wound. One of codeine known side effects is constipation…
After 12 days, the site is closed. Granulation tissue covers the centre of the wound. Keratinized gingiva covers the crown. Traction on the metal ligature wire is initiated. An elastomeric chain ensures a vertical traction force posterior to the impacted canine.

Healing after 44 days
Healing after 44 days shows keratinized gingiva reappearing in the former site (green arrow) and the apically repositioned band of gingiva (blue arrow) healed well. The elastomeric chain was replaced by a new one and the metal ligature wire was shortened and bent.

When the flap is replaced to its former position, traction is done blindly and the metal ligature wire or the cleat can come out through the mucosa or through the gingiva gradually as healing and traction occur as shown in the figure on the opposite side. This perforation of the gingiva determines the quantity of keratinized gingiva that will cover the neck of the tooth.

Comparison between 2 canines in the same patient. The left canine erupted normally. The right canine, which was impacted, presents a narrow band of keratinized gingiva.
The image on the opposite side shows well the difference between the bands of keratinized gingiva comprised between the blue and black arrows when the canine erupts normally on the left, compared to when the ligature cleat perforates the mucosa right below the mucogingival junction. The right canine shows only a little gingival festoon and little or no keratinized gingiva at the neck of the tooth. A free autogenous graft will likely be necessary in the medium term. The length of the left canine is different from the right one because keratinized gingiva covering it has not finished its migration upward. The patient is only 14 years old. The right canine, however, should not get any longer because the gingival attachment is located at the cementoenamel junction.
An open surgical approach with pediculated connective tissue graft (apically repositioned flap) as recommended by Vanarsdall (Sem.Orth. 2010) would have resulted in a better band of keratinized gingiva at the neck of the left canine.
Hi Dr. Sylvain. My 13 yr old had laser surgery 1 year ago to expose her palate ectopic canines. One is coming down more than the other and the ortho has discussed pulling them and putting implants in or not having canines altogether. I’m thinking of getting a second opinion as I don’t want to give up. You can see them in the palate, but the progress has been slow. Your thoughts?
You should initiate orthodontic traction of the impacted canine. I would not wait they erupt by themselves any longer. I am not sure what you mean by implants. I hope it does not mean to remove the canine and replace them by dental implants.
At 13 years old, it is not that difficult to bring the canine into occlusion if there is adequate space.
Hi,
Our 10 yr old has left upper canine/pre-molar transposition. Is it possible to avoid extraction of permanent teeth?
Are you able to give referrals for our area?
Thank you
Jon & Caroline
Having a transpostion do not mean that it will end up with extraction of permanent teeth. However, it might be necessary to manage the eruption of the transposed teeth by extraction of primary teeth.
I am quite sure it would be too early to take the decision to extract permanent teeth because of the transposition, but it is not imposible that once in permanent dentition, extraction could be a treatment option.
It is hard to tell with so little information.
Your IP address indicate that you likely live in Hawaii. I don’t know orthodontist in your area, but I am sure there are many good one.
Hi doctor hope you doing well, I’m going to ask you how can we determine that canine has bucally or palatally impacted only with panoramic radiogaphy.please guide . Thanks for your time
Palatal impaction
In the picture on the left, one can see the root of the incisors superposed with the crown of the canine and we can palpate the bilge in the palate. This mean that they are palatal.
When the canine are impacted in a vestibular position, the crown ot the lateral incisors are often displaced labially because the canine is buccal to their root. The palpation will reveal coving buccal to the laterals.
I hope that help.
Hi there!
I’m 25 and having surgery on one of my canine teeth and I’ve been doing reading about the subject and authors keep noting that the teeth can naturally erupt after surgery and packing of the tooth. They also talk about placing something on the tooth causing it to erupt naturally??
I’m just wondering if you could confirm if this happens with people my age or are they likely just talking about rectifying the problem early with 10-12 year old and catching the end of the eruption period.
.. Could my impacted canine naturally erupt at my age with a little force and guidance?
Your impacted canine will erupt if a force is apply via an attachement bonded on the crown and a chain or a ligature to transmit the force. It can make some self eruption if it is exposed and leaved uncovered (open eruption technique) but it wont go into alignment by itself.
Hello! My 15 yr old son has “one” impacted maxillary canine that is palatally impacted; primary tooth is gone.
His situation has been called the best case scenario (angle of impaction, no roots resorbed, straightforward impaction). However, with no decidious canine remaining, the lateral and centrial incisor have been drifting and the gap for the canine is only @2-3 mm at this point.
What would be your recommended first step?
1. Braces first; see oral surgeon months later to expose the impacted tooth
2. Or, see the oral surgeon first and then, a few weeks later, have braces installed
Thank you for your time!
I would recommend that you see the orthodontist first. He will plan the sequence of treatment. Chances are that space regain may be require to fit the canine into the arch. My preference is to have braces on or a removable appliance ready to fit in once the surgical ligature is done. I begin the traction one weeks after surgery.
Thank you so very much for your response! He did place the gum flap above the descending tooth afterall. I could not see it because he used glue instead of stitches to secure the gum. I am hoping all goes well. I truly appreciate your help!
So everything should be fine. Keep us informed.
My daughter had both of her canine teeth impacted. She had surgery today to pull them from her gums. However, the surgeon did not leave any keritinized gum in place. He cut away all of the gum to expose the teeth and attach them to her braces. I’m concerned now that she will not have sufficient gum coverage as the teeth decend into place. Should I be concerned like this?
If the surgeon placed the gum above the crown using an apically repositioned flap, don’t worry. The gum will follow the canine as it erupts.
If he cut a window in the gingiva, it is not good, but a keratinized gingival graft can be done at the end of the ortho treatment.
I hope that help. You can send picture via my facebook professional page account.
Palatally impacted canine open exposure surgery on 15 year old: does patient need IV sedation or would Valium and numb the area sufficient? How long will post op pain last and how long before eating normal food? Thanks.
It depends on the patient anxiety and the surgeon.
Generaly, local anesthesia is sufficient. But some patients who have high anxiety may benefit from IV sedation.
Pain may last for a few days, 2-4 days. Soft diet may be recomemnded for 1 week.
Dear Dr. Chamberland,
My son had the procedure to remove 4 baby teeth and expose the canines on the palate side. They are impacted. This was 1.5-2 months ago. The perio packing has now fallen out on both sides while eating cheerios and a toasted roll. Is the normal? After 2 trips to repair one side then the other, it happened again. The surgeon now say to go back to the orthodontist because the teeth may be erupting. Do you think the exposure procedure can work in just 2 months?
Thank you
Michael
Canine exposure and perio packing
Yes.
You can see at the beginning of this page a case from a collegue in Ontario. This is a good exemple of healing with a perio packing.
The goal of a perio packing is to obtain healing of the palatal mucosa without recovering the impacted canine. Ususally, I removed the perio packing 10 to 14 days after the surgery and I initiate immediately the orthonontic traction qith either a removable or a fixed appliance.
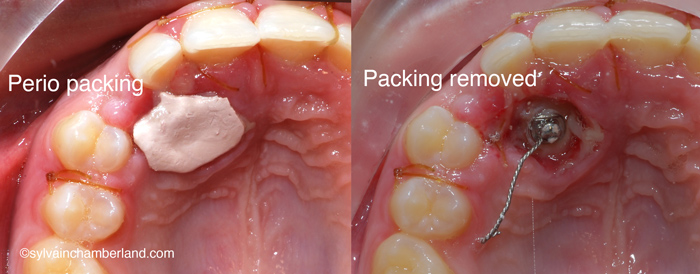
In this case, when the patient came, it might be 7-10 days after surgery. I removed the packing and i was ready to intiate the traction because the surgeon had bonded a button and attached a wired ligature.
The follow up of this case show a good healing and the canine remain visible, not covered by gingival tissue at 2 and 4 monhts.
At 4 months into treatment, I had to change the biomechanic. Theferore i used fixed appliances from this moment.
Hello, I am a 20yo female impending surgery to have my impacted canine exposed. It is in the palette of my mouth. Roughly, how long would I have a gap for once the baby tooth is removed? I am very self conscience about this whole procedure and treatment
There is no free lunch.
Depending how far in the palate your tooth is, it may take 6 month to 1 year to get the canine in the space. However, the whole wille not look like a whole as the tooth will be approaching.
No worries, at the end of the treatment, your canine will be nicely aligned.
Best regards
There is many ways to bring an impacted canine into occlusion and the one you describe is one of them. However, engaging a Niti wire to the attached chain is likely to cause side effect of intrusion and canting the occlusal plane even if the tooth in not ankylosed. The figure on the left show the force system and what occurs in picture A and B. The recommended approach is to use a main rigid archwire and an auxilliary wire (picture C). The main arch wire will prevent side effect and the auxilliary wire will assist the forced eruption.
My preferred approach is to use a removable appliance so there is almos no side effect on the adjacent teeth. Once the canine has moved and is visbile in the mouth, then i will finish the cases with braces.
I have limited experienced with luxation of an ankylosed tooth since often time it reankylose as it healed and it may undergo external root resorption. Therefore this is not my preferred option, but i know some orthodontist did it.
A more complete answer would take me 1 hour to write, but all my materials is availables in keynotes. I recommend that you look at the keynote palatally dispaced canine in my slideshare site.
I was lecturing at NYU College of dentistry last Firday (May 1st) and the first 15 minutes of the lecture was on mechanics to extrude high canine. Most slide are in the above mentionned keynote
I hope that help.
Best regards
Hi Dr. Chamberland.
I reside in NYC. I am a 34 y/o undergoing ortho treatment 18mos and traction on an upper right canine for 4mos.
A periapical taken recently didn’t show any noticeable canine movement. It is sitting in a vestibular position, but the very tip of the crown is out of the bone labially, where the oral surgeon attached the bracket and chain.
My Ortho currently has a Niti wire going through the arch up through a link in the attached chain.
I feel soreness constantly but can’t feel or see any visible results.
If it is ankylosed, I want someone knowledgeble to definitively diagnose it radiologically (PDL juncture), and/or using the percussion method.
Also, if we can determine how much of the tooth surface is fused, and if it’s a small percentage, if subluxation would be an option.
If it’s not ankylosed, I am concerned if my ortho understands why it got impacted in the first place, as I had an over-retained baby canine until I was 25, and if he is applying the right force or understands the anchoring demands to move this tooth.
My last visit 2wks ago, he noticed some intrusion of arch. He said that’s a bad sign 🙁 I am desperate to have this tooth come in, because of the time, cost, possible risks with extraction, grafting, and implant.
I have xrays and photos if you wish to see them. I would appreciate some advise. I am grateful for your thoughts and ideas!
I have impacted canine abv my lateral incisor my orthodontic is telling me for surgical exposure should I go for it? How long it will take to erupt
Of course you should go for it. It may take 6 to 12 month to bring the canine into occlusion.
Treament time is dependent of the initial position of the impacted canine, the exposure approach, the mechanics that is used and the skills of your orthodontist.
I’m 25 with two impacted cainines in the roof of my mouth. One is fully erupted and the other is partially erupted. Will the partially erupted tooth be exposed enough to move in place by braces? Or since they have been stuck in this position for about ten years will braces even move them over?
No, I would not worry. Braces will bring your teeth in alignment assuming adequate treatment plan and mechanotherapy is used.
I have question, when we will do open or closed technique? And when we should extract?
Thanks dr
Open technique should be the preferable approach for canine exposure as describle by Kokich, Semin Orthod 2010; 16: 205-211 and Vanarsdall, Semin Orthod 2010;16:212-221.
About your question : when we should extract?
The answer is: You extract every time when it is indicated.
My orthodontist is having a difficult time pulling an impacted cuspid thru the bone/tissue. He now wants to make small punctures into the bone that will soften this area in order to pull it out. Apparently, my oral surgeon put the exposure bracket on the wrong side. Is this a common procedure? Is it painful?
I agree with an exposure of the crown of your impacted canine. I doubt that the oral surgeon put the bracket on the wrong side. Once the canine is exposed, he can put it only in a place where he has access. If the tooth is rotated, the orthodontist qill derotate it when he can rebond the tooth.
Surgical approaches shown in this page are fairly common and not that much painfull. Of course you may have to take some advil or tylenol the 1st week.
I had expose and bond procedure with a open hole in the roof of my mouth. Little over a week out and the hole has filled with hard dark tissue. Is this normal
Yes, it is normal. It may be blood clot and granulation tissue. This tissue may cover the exposed canine.
i have impacted canine behind my two incisor teeth and it is slanted by 45 degrees.. are there any way to positioned my canine tooth…
Yes, there is a way to get your canine into dental arch alignment.
This case show an impacted canine (23) at baseline in March 2013. The primary canine (63) was retained and there was a periapical lesion (granuloma) depicted by the dashed line.
The canine was surgically exposed and a button was bonded on the crown like show in the surgical techinique above. A force was applied through a cantilever spring soldered on the Adams clasp of the removable appliance. The picture of march 2013 show the evolution at 1 year. I saw this patient yesterday and the button is exposed through the gingiva. In 2 weks or so, I will bond the brackets on every teeth and continue the treatment until the canine is aligned. I expect one more year of treatment to finish the case and debond.
.
i was having a impacted canine on right side upper jaw.i was experiencing shock like pains in my complete right side in both the jaws.it was surgically extracted and it took 5-6 months to get cured.still i feel painful sometimes while eating in my lower jaw .i wanted to know will it be cured permanently or not.how long will it take?
The pain you describe “shock like pain” in your complete right side of both jaws indicate me that the source of your pain might not have been “the impacted canine”.
I am very surprise that it took 5-6 months to cure. Usually, it is 1-2 weeks.
If you are still experiencing pain in the lower jaw, may be you should look for dental caries, pulpal tooth infection.
You need to see a “good” dentist.
Best regards