Wisdom teeth
Did you appreciate the information?
 (1 votes, average:moyen: 5.00 out ofsur 5)
(1 votes, average:moyen: 5.00 out ofsur 5)Introduction

Third molar and retromolar space
Third molars are commonly called wisdom teeth because they erupt in the mouth around 16-18 years of age. They are the last teeth to erupt and the available space to accommodate them is often limited. It is thus not surprising that these teeth can either not erupt completely, or not erupt at all. Thus, we say that they are partially or totally impacted.
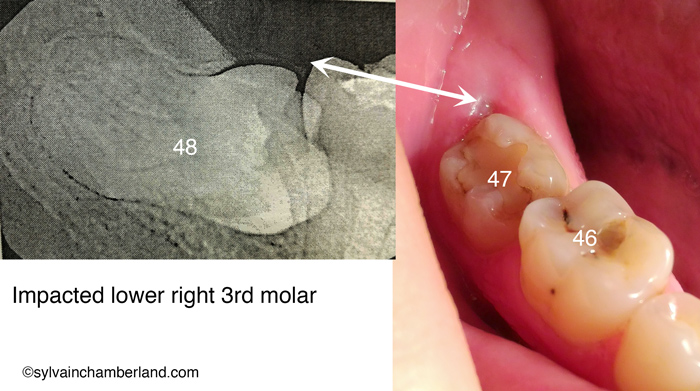
The X-ray on the opposite side shows the presence of 3 molars (first, second, third) which are aligned correctly. On the left of the third molar, arrows indicate the available retromolar space horizontally (white arrow) and vertically (red arrow). This space is essential to maintain optimal oral hygiene in this area to avoid the accumulation of bacterial plaque and pathogenic bacteria that are responsible for dental caries, periodontal pathology or both.

Intraoral view of lower molars. The third molars are commonly called wisdom teeth.
The picture on the right presents an occlusal view of the 3 molars from the previous X-ray.
The most posterior portion of the third molar is at the same level as the gingiva of the retromolar pad. It is essential to floss at the back of this last tooth to prevent the accumulation of subgingival bacterial plaque.
In the case presented, there is no inflammation or bleeding in that area, thus no periodontal pathology. There is also no evidence of caries.
This picture is representative of a wisdom tooth that is “asymptomatic” and “without pathology”.
Third molars and incisor crowding
It is an old controversial subject, but we can say that there is no convincing scientific evidence showing that third molars can cause incisor crowding (make teeth crooked).
Harradine N.G. and Pearson M.H. (BJO/vol25/1998/117-122) recruited 164 patients having received an orthodontic treatment and having third molars. After a period of more than 5 years, 77 patients were examined again. 44 patients had their third molars extracted, 33 had kept them. The incisor crowding was compared between these 2 groups.
The crowding measured by the irregularity index shows that this index is 1.1 mm for the group who had their third molars extracted and 2.1 mm for the group whose third molars were not removed. The difference of 1 mm in favor of the group with the extracted molars is not statistically significant (p = 0.15). The difference is not considered as clinically significant. This prospective, randomized, study concludes that the prophylactic extraction of third molars to reduce or prevent incisor crowding cannot be justified.
The conclusions of this study are in line with the conclusions of the study conducted by Lindquist and Thilander (AJODO 1982; 81, 130-139) and that conducted by Vego (AO 1962, 32, 187-192) who found a very small increase inincisor crowding if third molars are present without being clinically significant.
Ades A.G., Joondeph D.R., Little R.M. and Chapko M.K. (AJODO 1990;97:323-35) observed incisor crowding in 4 subgroups.
- Both lower third molars erupted to the occlusal plane
- Bilaterally impacted third molars
- Bilateral agenesis of third molars
- Bilateral extraction of third molars since at least 10 years ago
Even if each of the subgroups showed incisor crowding, no significant differences of crowding could be observed between each of these subgroups. The authors concluded that the prophylactic extraction of third molars with the objective of alleviating or preventing mandibular incisor irregularity may not be justified.
Symptomatic versus asymptomatic
Young adults would really like to know if their wisdom teeth which do not show any symptoms – asymptomatic – (no pain, no caries, often impacted and in development) also have no pathology. They would also like to know, if their third molars do not have any pathology at present, what are the chances of having any problems with their third molars if they keep them throughout their life.
Third molars that do not show any symptoms can be associated with cysts or tumors (odontogenous tumors) and mandibular fractures. However, the prevalence of these problems is low, probably less than 5%.
We find pericoronitis (infection around the tooth crown) and periodontal pathology (periodontal pockets, bleeding, bone loss) in patients who have symptomatic third molars. These chronic conditions, or conditions with acute episodes, have a prevalence of about 10%.
Prevalence of third molars with a carie or a periodontal pathology
A longitudinal study convened by 2 academic centres, University of Kentucky and University of North Carolina, has just been released studying the prevalence of pathologies associated with third molars.
409 healthy individuals, of 25 years of age on average and having 4 asymptomatic third molars participated in this study. The periodontal health was evaluated with the “probing depth” parameter. A probe graduated in mm is inserted between the tooth and the gingiva. If the measure is greater than 3-4 mm, a periodontal problem exists.
Periodontal pathology
55% of the individuals had at least one probing site of 4 mm or more around the third molars while 23% of the individuals presented at least 4 probing sites of 4 mm or more around the third molars. The lower third molars were most often affected by probing sites of 4 mm or more.
Of the 229 individuals having all their third molars in occlusion, 72% had at least 1 probing site of 4 mm or more.
Another study (Blakey, Maricani et al, JOMS2002;60:1227) of 329 asymptomatic individuals showed that 24% of asymptomatic third molars had at least 1 probing site exceeding 5 mm. Yet, a probing depth of 5 mm is associated with a 2-mm attachment loss.
Dental caries
24% of the individuals presented third molars with caries experience whereas caries on the first and second molars occurred in 73% of the individuals.
Only 16% of the individuals had third molars free from caries or periodontal pathology.
What is your advice to patients about their third molars?
Not having any symptoms does not mean not having pathology (diseases).
The risk marker (pocket > 4 mm) cannot be ignored in the development of potential pathology around third molars. Chances are that, even without symptoms, periodontal pathology around third molars can get worse with time and that other teeth located anteriorly to the third molars will be affected.
The prevalence of caries presents a different model. Third molars are rarely affected by caries without having the first or second molars already affected.
Experienced clinicians know that the surgical extraction of third molars and the recovery after the surgery are more difficult if the extractions are done in adulthood (> 21-25 years of age).
Philip et al (AJODO 2010;138:700.e1-700.e8) showed in a study on 958 individuals that recovery is faster after a surgical extraction of third molars in younger individuals. Patients being less than 21 years of age, including teenagers who completed an orthodontic treatment, recover more readily depending on the “quality of life” parameters: lifestyle (social life, hobby), oral function (eat, chew, open the mouth) and pain than patients who had their extraction after 21 years of age. Moreover, boys recuperate easier than girls.
Decide to extract or to keep and monitor?
The decision to extract or to keep the third molars must be made by the patient after getting the best information possible.
The decision to extract implies for the patient a surgical procedure under local anesthesia. Risks are well known and documented and the recovery is related to perioperative difficulties of the surgery (easy vs difficult) and the age when the surgery is performed.
The decision not to extract means periodic monitoring involving a clinical and radiological examination and more unknowns about the long-term result.
Based on data from recent studies, 70% of young adults with asymptomatic third molars already have an existing pathology or will develop a pathology.
Inversely, 30% or less of young adults will not have pathologies associated with their third molars.
A decision to not extract means keeping these teeth and accepting the risks associated that may develop with it with age.
Guideline-indications to extract
• Presence of symptoms
• Presence of radiological or clinical signs of a pathology
• Another dental pathology or general systemic disease (diabetes)
• Preventive (prophylactic) extraction
• Horizontal, vertical or distoangular tooth not totally buried in bone
• Incomplete formation of roots, but showing a risk of touching the nerve once the root formation is complete
Clinical examples
Pericoronitis

Pericoronitis around a wisdow tooth. Chronic infection (arrow 2) and presence of pus (arrow 3).

Chronic infection site causing pericoronitis (white arrows).
The picture on the left shows a wisdom tooth that we could consider as “asymptomatic” in the sense that it did not cause any pain, but presenting with chronic infection revealed by the purple-blue color of the gingiva covering the occlusal surface (arrow 2) and the presence of a purulent green fluid exuding from under this gingiva (arrow 3). Therefore, a pathology exists.
The X-ray on the right shows the extension of the bone destruction caused by this chronic infection.
The patient is 32 years old and the infection has been active for probably ten years or so.
Chronic infection can degenerate into an acute infection at any times and it is generally not the right time nor the right place when it happens. Imagine an acute dental infection while on a trip down south or the day before a long time off…
This wisdom tooth clearly has to be extracted and that’s what happened.
The extraction of partially impacted molars prevents the formation of postoperative periodontal pockets. The prevalence of teeth at risk of developing a pericoronitis is of 36%.
Other examples of wisdom teeth at risk of pericoronitis

Partially impacted wisdom tooth #48.

Partially impacted wisdom tooth #38 and radiographic view.
.
Here is a 21-year-old young patient. His left and right wisdom teeth are partially impacted and vertically positioned.
The part of gingiva that covers it is called the operculum. The white dotted lines on the X-rays indicate the amount of soft tissues covering the occlusal surface of the tooth. The black arrows outline the extent of the lesion at the bone level. I invite you to compare the extent of these lesions at the bone level with the one of the 32-year-old woman in the above image.
Partially impacted and mesioangular wisdom teeth

Evolution of wisdom teeth in a young man of 19 years of age (in 2008) and of 21 years of age (in 2011)
This young man was almost 19 years old at the beginning of his orthodontic treatment. He had been warned about the poor prognosis of his wisdom teeth eruption of and he had been informed that their extraction would probably be necessary at the end of the orthodontic treatment that had involved the extraction of 4 permanent premolars.
At the end of the orthodontic treatment, the angulation of left third molar improved (became more upright) and was able to erupt. However, this was not the case on the right side. The tooth, mesioangular, remained trapped under the height of the edge of the second molar and it did not have enough space between its distal aspect and the ramus of the jaw to upright.

Mesioangular wisdom tooth.
Clinically, the right color picture shows that the occlusal surface of the tooth is tipped forward (mesioangular). The zone indicated by the white arrows is hard to clean. Food builds up, facilitating the development of a caries both on the wisdom tooth and the second (2nd) molar.
Dental caries caused by a mesioangular wisdom tooth

Dental caries caused by mesioangular wisdom teeth
These X-rays show big cavities (white arrows) which develop when a mesioangular wisdom tooth is left evolving in partial eruption. The difficulty in cleaning this type of food trap guarantees development of large caries in the future and with possible loss of, not only the third molar, but also the second molar or having a root canal treatment with an expensive restoration to save the second molar.
Back to top.
Root near the inferior alveolar nerve

Root of third molars in development and near the inferior dental (alveolar) nerve.
The prevalence of roots of third molars that grow near the dental nerve is of 26%. This means that one out of four third molars is at risk of having roots touching or surrounding the dental nerve when their formation is complete.
The X-ray on the opposite side shows third molars where the development of the root is near the inferior dental nerve in a 17-year-old young man. As the roots will continue their development, they will surround the nerve. The prognosis for eruption of these teeth is poor. One is mesioangular and touches the second molar (black arrow). This means a risk of caries or pericoronitis at 20-25 years of age if the molar only partially erupts. To avoid having the risk of causing damage to the nerve if the extraction is done at 25-30 years of age, we proceeded to the prophylactic or preventive extraction of these wisdom teeth.

Root of third molars in contact with the inferior dental nerve
Here is the X-ray of a 24-year-old young woman. The formation of the roots of the third molars is completed. The dental nerve canal is outlined by the black dotted line. The extremity of the roots, indicated by the white arrows, crosses the dental canal space. These molars are totally impacted and are asymptomatic. There is a high risk of paresthesia (damage to the dental nerve) following surgical extraction.
Here is the kind of case where it is too late to do anything and it is better to monitor the evolution with an X-ray taken every 2 years. The complete extraction of these wisdom teeth is thus not recommended. A partial odontectomy would be more recommended approach.
Partial odontectomy

Partial odontectomy. Notice the excellent bone regeneration which allowed covering of the root of the second molar.
Here is an example where roots of a wisdom tooth surrounded the dental nerve and crossed the dental canal. It was decided to cut the tooth crown (partial odontectomy) and to leave the roots in place (surgery performed by Dr Jean-Philipe Fréchette, oral and maxillofacial surgeon). Subsequent X-rays show excellent healing and bone regeneration that allowed the covering of the distal surface of the root of the second molar.
Odontogenous cyst

Odontogenous cyst around the crown of the lower left wisdom tooth
The enlarged follicular envelope around the crown of the impacted tooth is representative of a dentigerous or follicular cyst. As the cyst gets larger, it will push the tooth deeper into the bone.
The roots of this molar cross the dental canal.
We are facing two risks:
• Risk of progressive development of the cyst
• Risk of paresthesia during the extraction
However, complications and risks associated with the development of the cyst overcome the risk of paresthesia of the dental nerve. In this case, a partial odontectomy. The surgeon cuts the tooth at the radicular trunk and removes the crown and the cyst. Therefore, the roots stay in place without nerve damage.

Dentigerous cyst in a 59-year-old man. Courtesy of Dr Carl Bouchard, oral and maxillofacial surgeon.
If some people wonder how large a dentigerous cyst can become, here is an example of a follicular (dentigerous) cyst in a 59-year-old man, that is about thirty years later than the previous dentigerous cyst.
Notice the movement of the tooth downward. The roots are superior to the lower edge of the mandible. It is certainly an extreme case and a marsupialization of the cyst first needed to be performed to decrease its size before proceeding with the extraction of the tooth and the cyst. Courtesy of Dr Carl Bouchard, oral and maxillofacial surgeon.
Periodontal pathology and wisdom teeth

Periodontal pathology and wisdom teeth. 1- inferior bone level. 2- superior bone level. 3- periodontal pockets of 4 to 5 mm. 4- roots in contact with the dental nerve. White dotted line: dental nerve canal. 29-year-old patient.
When a wisdom tooth is totally impacted, it is important to verify that there is no communication between the oral cavity and the follicular envelope. In the case shown on the opposite side, communication exists right at the back (in the distal) of the second molar. Inserting a periodontal probe in sites indicated by arrow 3 shows a pocket of 4-5 mm, which means that the extremity of the probe reaches the crown of the impacted tooth. Bleeding occurs when probing, which also means that there is chronic inflammation and that these sites cannot be totally cleaned with dental floss.
The root of the second molar is in contact with the crown of the third molar and there is no bone covering this part of the root. The bone level should normally be at the level indicated by arrow 2, but it is much lower, as indicated by arrow 1.
Moreover, the roots of the wisdom teeth are in close proximity to the inferior alveolar nerve (arrow 4).

Periodontal abscess caused by a chronic infection.
Chronic infection near the root may evolve into a chronic abscess leading to important bone destruction occuring on the distal of the second molars along with root caries. This can mean the loss of the second molars.
The X-ray on the opposite side shows well the additional bone loss (between arrows 1-4) caused by a chronic periodontal infection which originated from a pocket in the distal of the second molar (arrow 3).
It goes without saying that the extraction is indicated in this type of case. Healing of the extraction site has to be followed clinically and monitored radiologically to ensure a good bone regeneration. Montero et al (JOMS 2011) demonstrated that one year after the extraction of third molars, the periodontal status in the distal of the second molar had greatly improved. The depth of the average pocket was only 2.6 mm instead of 4-5 mm.
Obstacle to the eruption of a second molar

Failure of eruption of second molars and overlapping third molars
When second molars present delayed eruption or when they are tipped mesially (forward), the best option of treatment is the extraction of the wisdom tooth.

Favorable evolution and eruption of second molars
The X-ray on the opposite side shows the uprighting of second molars. Molar #38 (right image) has erupted. Tooth #48 (left image) has erupted, but is still subgingival.

Eruption of tooth #48
10 months later, tooth #48 has come out of the gingiva sufficiently to bond a bracket to it.
.

Final evolution. The second molars are in good position.
The final result shows second molars in good position with the interradicular bone level being entirely generated.
Rescue of the third molar

Heavily restored first molar and rescue of the third molar.
The case on the opposite side shows a first molar with an extensive carie and a vertically partially impacted third molar. To achieve the overall orthodontic treatment goal, dental extractions had to be performed. In this case, instead of choosing a healthy second premolar, I decided to extract the damaged first molar (X) to save future expensive restoration fees.
The second and third molars were protracted (brought forward). Notice the available space (black arrow) at the back (in the distal) of the third molar at the end of the treatment compared to the available space before the treatment.
The third molar is no longer in the ramus and now it is easy to keep this area clean, without infection.
Extract these ones, wait for those ones
At the end of an orthodontic treatment, the orthodontist must generally give his opinion on extracting or keeping wisdom teeth. Patients are mostly teenagers from 12 to 17 years of age. At this age, only one third of the roots of wisdom teeth is developed and it is normal for them to be “impacted” without presenting any pathology. The orthodontist’s role is to evaluate the risks by asking the following questions.
1- Does the third molar have a chance to erupt? Poor or favorable prognosis of eruption?
2- Does the third molar have enough space to erupt wihout incident?
3- If it erupts, will there be enough space for the crown to be completely emerged from the gingiva or will it be partially covered by gingiva?
4- Does the root, while developing, have the risk of surrounding or be in contact with the dental canal or nerve?
To illustrate these questions, I present two boys: one of 16 years and 3 months of age and the other one of 15 years and 8 months of age.

Indication of wisdom teeth extraction. Boy of 16 years and 3 months of age.
On the left, here is the boy of 16 years and 3 months of age. The prognosis for eruption ofthe wisdom teeth eruption is poor to nil. They are in contact with the roots of the second molars (black arrow). The space between the second molar and the ramus (white arrow) is insufficient to accommodate the crown of the wisdom tooth. The roots are not in contact with the nerve, but it is easy to imagine that they have the risk of being in contact when development is complete.
In this case, it is unnecessary to wait to see the outcome, it is preferable to extract the wisdom teeth now.

Wisdom teeth that we can monitor and reevaluate in 18-24 months. Boy of 15 years and 8 months of age.
On the right, the boy is 15 years and 8 months of age. The prognosis for eruption is uncertain. The space between the second molar and the ramus is surely limited to accommodate the wisdom tooth, but it does not touch the second molar. There is a 2-3 mm space (black arrow). The roots are a little less developed than the other boy. The difference in development is observed by the radicular furcation which is less developed and the roots are comparatively shorter.
It was decided to wait and monitor the development. A radiographic reevaluation will be done in 24 months.
Mandibular osteotomy and removal of third molars
Alteration in the sensitivity of nerves immediately following a mandibular sagittal split osteotomy is observed in 80 to 100% of cases. Sensitivity is recovered in the subsequent months, but a certain number of patients can remain with a loss of sensation due to an inferior dental (alveolar) nerve injury (paresthesia, dysesthesia, hyperesthesia). The presence of third molars during this kind of surgery is considered as an additional risk factor.
The presence of third molars could also be associated with a bad split during the osteotomy. That is why it is generally recommended to proceed with the extraction of third molars before undertaking a mandibular osteotomy and it is common practice in the Quebec City area. It is also common practice at the Universities of Toronto and Montreal.
From the point of view of research and convincing evidence, here are thus 2 questions that we can scientifically verify.
1- Does the presence of a wisdom tooth during a mandibular osteotomy increase the risk of nerve injury (paresthesia)?
2- Does the presence of a wisdom tooth increase the risk of a bad split during a mandibular osteotomy?
Therefore, the oral surgery group at Dalhousie University in Halifax conducted a study with a prospective study to address these questions and they demonstrated that the risk of having a nerve injury or a bad split was not increased when the third molars were present during an osteotomy than when the third molars were not present.
Indeed, Doucet JC, Morrisson AD et coll. (JOMS 2012) conducted a prospective study with 677 patients having undergone a mandibular sagittal split osteotomy (MSSO) divided into 2 groups.
Group 1 consisted of 331 MSSO for which the third molars were removed during the surgery (concomitantly). Group 2 consisted of 346 MSSO where the third molars were congenitally absent or removed at least 6 months prior to the surgery.
The rate of bad splits was of 2.4% in group 1 ( third molars present) and of 3.8% in group 2 (without third molars). Although the rates are different, there is no significant difference between the two groups (p = 0.315).
The rate of nerve injury (paresthesia) was less in group 1 (with wisdom teeth) than in group 2 (without wisdom teeth). In group 1 (with wisdom teeth), 70% of patients had regained their normal sensation in the lips 3 months after the surgery and 90% of patients had regained their normal sensation 6 months after the surgery. In group 2 (without wisdom teeth), 48% of patients had regained their normal sensation in the lips 3 months after the surgery and 68% of patients had regained their normal sensation 6 months after the surgery. There is thus a significant difference in favor of group 1 (with wisdom teeth) in terms of regaining their normal sensation in 3 months (p = 0.031) and in 6 months (p = 0.009).
However, we must examine the demographic characteristics of the groups under study. Group 1, the one with third molars, was in average 19.6 ± 7.4 years of age whereas group 2, the one without third molars, was in average 30.04 ± 12.1 years of age. These two groups are significantly different (p < 0.001).
It is probably fair to say that roots of wisdom teeth are less developed in a group where the average age is 19.6 years compared to a group where the average age is 30 years. It can also lbe postulated that it is more difficult for a 30-year-old adult to recover from orthognathic surgery than a 19-year-old young person.

Effect on the presence of mandibular third molars during a mandibular sagittal split osteotomy (MSSO) depending on different age categories. Doucet et al, The Presence of Mandibular Third Molars During Sagittal Split Osteotomies Does Not Increase the Risk of Complications, J Oral Maxillofac Surg 70:1935-1943, 2012
Table 6 on the opposite side divides the experimental groups into age categories.
1- Age < 20 years: for patients who are younger than 20 years, there is no significant difference between groups 1 and 2 concerning unfavorable fractures and alveolar nerve entrapment.
2- Age between 20 and 30 years: There is no difference between the 2 groups about bad splits, but there is an increase in the frequency of nerve entrapment.
3- Age > 30 years: There is no difference between groups 1 and 2 in terms of bad splits or nerve entrapment, but it takes longer to perform the osteotomy if the third molar is present.
Nerve entrapment means more manipulations to release the nerve between the proximal and distal segments once the osteotomy is performed. This does not mean, ipso facto, that a loss of sensitivity in the lip will occur.
In conclusion, the decision to extract wisdom teeth prior to an orthognathic surgery must be discussed with both the orthodontist and with the oral surgeon who will perform the procedure.
Osteotomy after the extraction of third molars

Horizontally impacted wisdom tooth extracted 15 to 18 months prior to the mandibular osteotomy.
Here is an example of a 33-year-old woman whose third molars were extracted 15 to 18 months prior to mandibular sagittal split osteotomy. The X-ray on the opposite side shows the horizontal impaction of the patient’s left third molar. The nerve and the dental canal are outlined by the black dotted line.
The oral surgeon used 2 bicortical screws and a monocortical chain plate for the fixation.

Extraction in preparation for orthognathic surgery involving mandibular advancement
Here is a typical example of a case (age at surgery = 17 years 8 months) where the third molar was extracted a minimum of 6 months prior to the orthognathic surgery. Bicortical screws are used for the fixation of bone segments. Note the proximity of the screws compared with the extraction site (white dotted line).
One of the reasons given by oral surgeons in the Quebec City area but not evaluated by the reseach group in Halifax is the need to have bone fragments of an acceptable thickness.

Bicortical screws used in fixation of a mandibular sagittal split osteotomy (MSSO). White dotted line: approximate position of the site of a third molar.
The picture on the opposite side shows the approximate position (white dotted line) of a third molar compared with the osteotomy cut. Knowing that a wisdom tooth occupies a space of 10 x 12 mm in the bone, we can imagine how thin the residual bone walls are when they are removed periop (during the surgery). The screw indicated by arrow 2 would be located precisely in the site occupied by a third molar if it had been present. The thinness of the walls and the void left by the cavity could compromise the solidity of the screw. The site indicated by arrow 4 is a potential site to position a bicortical screw.
Thinness of cortical plate

Traumatic fracture of the mandibular angle Note the site occupied by the third molar and the irregular extension of the fracture. Courtesy of Dr Carl Bouchard, oral and maxillofacial surgeon.

Traumatic fracture of the mandibular angle. Fixation with a monocortical plate. Courtesy of Dr Carl Bouchard, oral and maxillofacial surgeon.
The concept of thinness and fragility of bone walls is perfectly illustrated in the following case where a patient experienced an impact causing a mandibular fracture. Notice the thinness of the walls near the site of the third molar when the fragments are brought together. A monocortical plate was used to achieve the fixation. We can also imagine or understand that the presence of an impacted third molar during the impact most likely increased the risk of fracture.
Mandibular osteotomy and simultaneous extraction of the third molar

Extraction of the third molar during the mandibular osteotomy. Oral and maxillofacial surgeon: Dr Jean-Philipe Fréchette
Here is the case of a young girl of 14 years and 6 months of age during her surgery. The wisdom teeth could not have been previously extracted. The screw in the center crosses the socketof the the third molar that was extracted at the same time as the osteotomy.
I discussed with the surgeon and he confirms that the screw went across the tooth socket. He confirms that it was firmly screwed. If it had not been the case, he would have put a monocortical plate.
Conclusion
1- Wisdom teeth are not responsible for the crowding or redisplacement of teeth following an orthodontic treatment.
2- Patients under 21 years of age, including teenagers who have completed orthodontic treatment, recover more easily when considering “quality of life” parameters: lifestyle (social life, hobby), oral function (eat, chew, open the mouth) and pain than patients who had their extraction after 21 years of age.
3- 70% of young adults with asymptomatic third molars already have a pathology or will develop a pathology.
4- An orthognathic surgery (mandibular sagittal split osteotomy) can be performed with or without the presence of third molars.
5- The presence of third molars during a mandibular sagittal split osteotomy (MSSO) makes the lingual and buccal cortical plates thin as a result of the void left by the tooth often making bicortical screws insufficient to immobilize the bone segments. A monocortical plate is then required.
Back to top.
Bibliography
White RP, and Proffit WR. Evaluation and management of asymptomatic third molars: Lack of symptoms does not equate to lack of pathology. Am J Orthod Dentofacial Orthop. 2011, Jul;140(1):10-6.
Phillips C, Gelesko S, Proffit WR, and White RP. Recovery after third-molar surgery: the effects of age and sex. Am J Orthod Dentofacial Orthop. 2010, Dec;138(6):700.e1-8; discussion 700-1.
Harradine W.T. The effect of extraction of thrid molars on late lower incisors crowding. British Journal of Orthodontics. 1998;25117-122.
Koumaras GM. What costs are associated with the management of third molars? J Oral Maxillofac Surg. 2012, Sep;70(9 Suppl 1):S8-10.
Phillips C, and White RP. How predictable is the position of third molars over time? J Oral Maxillofac Surg. 2012, Sep;70(9 Suppl 1):S11-4.
Marciani RD. Is there pathology associated with asymptomatic third molars? J Oral Maxillofac Surg. 2012, Sep;70(9 Suppl 1):S15-9.
Pogrel MA. What is the effect of timing of removal on the incidence and severity of complications? J Oral Maxillofac Surg. 2012, Sep;70(9 Suppl 1):S37-40.
Ventä I. How often do asymptomatic, disease-free third molars need to be removed? J Oral Maxillofac Surg. 2012, Sep;70(9 Suppl 1):S41-7.
Garaas RN, Fisher EL, Wilson GH, Phillips C, Shugars DA, Blakey GH, et al. Prevalence of third molars with caries experience or periodontal pathology in young adults. J Oral Maxillofac Surg. 2012, Mar;70(3):507-13.
Montero J, and Mazzaglia G. Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar. J Oral Maxillofac Surg. 2011, Nov;69(11):2691-7.
Zhang Q, and Zhang Z. Early extraction- a silver bullet to avoid nerve injury in lower third molar removal? [Internet]. Int J Oral Maxillofac Surg. 2012, Mar 21;41(10):1280-1283.[cited 2012, Mar 21]
Falci SG, de Castro CR, Santos RC, de Souza Lima LD, Ramos-Jorge ML, Botelho AM, and Dos Santos CR. Association between the presence of a partially erupted mandibular third molar and the existence of caries in the distal of the second molars. Int J Oral Maxillofac Surg. 2012, Mar 30;
Rebecca Lash Rubin,a Tiziano Baccetti,b,y and James A. McNamara, Jrc West Bloomfield and Ann Arbor, Mich, and Florence, Italy, Mandibular second molar eruption difficulties related to the maintenance of arch perimeter in the mixed dentition, (Am J Orthod Dentofacial Orthop 2012;141:146-52)
Magnusson C, Kjelberg H, Impaction and Retention of Second Molars: Diagnosis, Treatment and Outcome A Retrospective Follow-up Study Angle Orthod. 2009;79:422–427
Montero J, and Mazzaglia G. Effect of removing an impacted mandibular third molar on the periodontal status of the mandibular second molar. J Oral Maxillofac Surg. 2011, Nov;69(11):2691-7
Doucet JC, Morrison AD, Davis BR, Robertson CG, Goodday R, and Precious DS. Concomitant removal of mandibular third molars during sagittal split osteotomy minimizes neurosensory dysfunction. J Oral Maxillofac Surg. 2012, Sep;70(9):2153-63
Doucet JC, Morrison AD, Davis BR, Gregoire CE, Goodday R, Precious DS. The presence of mandibular third molars during sagittal split osteotomies does not increase the risk of complications. J Oral Maxillofac Surg. 2012 Aug; 70(8):1935-43. Epub 2011 Dec 10.
Thank you very much for your answer. Probably, it will be removed. I do not know how, it will be decided today.
Hello.
I do not speak in English (writing via Google Translate).
I read your article on wisdom teet.
And I realized that you’re a real expert!
I live in Russia. The level of medicine we have a very poorly developed. It is very difficult to get professional help even for money. I wanted to ask you whether the Council should remove my wisdom teeth. I am 29 years old. I enclose a photo and X-ray of the tooth. It tried to make a good photo. Hopefully we will see. In the photo you can see a bit of what became erupt gums. The tooth does not disturb. Only the unpleasant smell of the place. Do you think whether it is necessary to remove the tooth. Or, you can not delete. The root of the tooth may touch a nerve – found out about this from your article. I’m afraid I will trust in our doctors. They can easily pull out a tooth without understanding. Please help advice.
Here is a photo:
Please tell me whether you can see on the x-ray shot that touches the nerve of the tooth? If the tooth should be removed, it is necessary to complete removal or partial removal of a tooth?
Sincerely, Eugene.
Hi Eugeny,
I would defenitely recommend the removal of the wisdom tooth. The white double end arrow indicate it is partially erupted. You can see 2 -3 mm of the tooth in the right picture that match with the xray on the left picture. This partially erpted tooth is at high risk of infection (periconitis) or causing decay or resorption of the root of the 2nd molar (#47).
However, the tooth may be at risk of causing nerve damage if the dental surgeon is not experimented. In Quebec, the removal of this tooth by an oral surgeon would not be a problem.
I hope that help.
hi dr, i just have a few questions
i’m 19 years old, and planning to get 4 wisdom teeth removed. 2 are partially erupt, all 4 cause discomfort, however.. they’re still growing.
1st, I was wondering, if i remove one wisdom teeth do i have to remove the opposing one?
2nd, i know when you remove a tooth, bone resorption occurs, so when you remove wisdom teeth, it happens to the back of your jaw as well. a lot of doctors claim there is no facial changes, but through my research i see many ppl saying they’ve noticed it. and apperently it takes about 18 months to start really noticing changes. so i was wondering if you can truthfully tell me is it possible that your face does collapse a bit?
3rd, is there irritation when chewing hard food, in the spots where the teeth are removed
4th, does bone grow back in the spot where the teeth is removed or is it just pure gum?
thanks for your time, hope you can reply.
1- Yes. If you remove one semi-impacted lower 3rd molar, you should removed the upper third molar.
2- The bone heal and you won’t have facial change.
3- You should avoid chewing hard food in the area of the removed teeth during healing.
4- The bone grow back.
Hi Dr Sylvain,
Thanks so much for this excellent article! So informative!
May I inquire, what should I expect after my dentist has left a root behind after removal of my upper right wisdom tooth?
1) Will the root eventually emerge years later and require removal?
2) Is there a risk of abscess formation?
This was her post surgical notes:
Excision of right wisdom teeth; impacted lower and non-functional upper right wisdom teeth
Operation done – Tooth (superficial), unerupted/partially erupted/impacted, excision with removal of bone and tooth division.
The root will likely become submerge and embed into the bone like in the case of partial odontectomy depicted above. It is often safer to let a residual root than try to dig bone around and take the risk to damage the dental nerve.
I would not worry about abcess formation. If it occurs you will need antibiotherapy anyway and the surgeon will be able to manage the complications.
From the written notes of your surgeon, i guees that he did a partial odontectomy on purpose. Chances are that he took the right decision.
Hi,
I was just wondering if you could clarify a concern I’ve been having over my extracted wisdom teeth. I have read conflicting opinion over whether their removal causes facial changes and was hoping to get a conclusive answer on this. These are some of the answers I’ve gotten from dentists and the like so far:
1) Yes, your facial profile will change. A slightly collapsing of the face will occur. (Dentist and Craniofacial expert in London)
2) Yes, bone remodeling will take place and the mandibular angle of the jaw will change. This will all happen over a few years. Also, Korean women commonly get them extracted to get a skinnier face. (Dentist in Korea)
3) Yes, changes can occur. (Customer service employee at the ADA)
4) And finally, no there will be no changes and the wisdom teeth have no affect whatsoever on the jaw and facial contours. (Almost every oral surgeon or dentist I’ve talked to in the United States)
Just wanted to get your thoughts on who I should trust/who would be correct in this instance..
Thanks so much for your time and expertise,
Victoria
I have never heard that the removal of of wisdom teeth would have any impact on facial profile, nor it may cause skinnier face.
I would trust American and canadian surgeon on this as well as my word.
Removal of wisdom teeth will not affect facial profile.
Question: I am a70 year old female with full dentures. I have a small hard, white eruption at the site of where a wisdom tooth would be. Swelling and tenderness evident.
Is it possible to actually have a tooth erupt at this age?
It is not impossible that you may have a remaining wisdomme tooth, but I would recommend that you visit a dentist and get a panoramic xray to confirm or infirm. It might be many other things that you could have. The wisdom tooth is likely the least probable.
A little remark about “extract these ones, wait for those ones”: around 18 years of age, according to Grobety and Pfeiffer, between the distal margin of the second molar and Xi of Ricketts analisys, must be 30 mm in order that the third molar find out its right position. Between 8 and 18 years the rule is: age + 21mm between the first molar and Xi. What think about thath? My best regards.
I know too few about Rickets analysis to comment on those numbers.
When i wrote this article, it was to provide general guides lines and to develop the clinical judgment on assessing third molars removal.
Rickets numbers might be ok for one particular case but if there is a perio pathology with the crown of the 3rd molars, who cares about Rickets value?
Best regards
Very nice presentation dr Sylvain, but I ve never done any partial odontectomy because I think partial odontectomy is very risky for not all patients could keep the area clean and healthy. And could cause an infected condition. So my decision is always perform a totally odontectomy, even the root is very closed to the mandibular canal, or encircling the nerve, but with a gentle and based of the previous cases, the rate of success almost satisfactorily.
Dr Goenawan,
Thank you for your kind remarks.
However, i disagree with your opinion on partial odontectomy. I am concern about your remark: “rate of success almost satisfactotily”.
Oral surgeons in my area do this approach qite often and they never encounter significant complications. If complications would occured, they are not different from the usual complication that occur with removal of wisdom teeth.
the recommended technique is to cut the crowm from the radicular trunk, then use a surgical round bur to grind the trunk some 5 mm below the margin of the alveole, suture the gum and let it heal.
most radicular trunk remain embeded in the alveolar bone. My surgeon who did several partial odontectomy in his carreer told me that he withnesses self- exfoliation. It was extremely rare.
the rate of success of partial odontectomy is “always satisfactorely.”
Best regards
Excellent and comprehensive review of the thought processes that must be exercised by clinicians and patients when making treatment decisions about third molar extractions. The examples are prudent and the information is well supported by the literature. I would hope that beurocrats who involve themselves in cost containment would have an opportunity to review your article.
Thank you Doctor Tillery for your kind remarks.
Great post with very logical and practical explanations.
S. Kent Lauson, DDS, MS, Orthodontist
Very nice comprehensive article Sylvain.
Whats your experience with partial odontectomies ?
Do you monitor long term periodically and are there any potential post-op complications?
Thank you Dr Aulakh for your comment.
Regarding experience with partial odontecomies, I did not saw that many cases during my orthodontic practice years. The main reason is that I am an orthodontist, not an oral surgeon.
However, I know this approach is often use by the oral surgeon in my area when the risks of causing nerve damage are high and the Xray (and nowaday a CBCT scan) show that the roots are circling or overlapping the alveolar nerve.
The case presented above in the section “root near the inferior alveolar nerve” show pictures 6 weeks after partial odontectomy and 19 months post odontectomy without any complication.
I went back to my patients file and found a 45 years old patient who had a mandibular osteotomy. If I recall correctly, I think the tooth was ankylosed so well that it was impossible to remove the tooth without causing aberrant fracture of the proximal or the distal segment.
The tooth was sectionned, the roots were removed but the crown was left in place. Follow up at 31 months post surgery show nice healing. No complications occurs.
I might have other cases in my files but it is difficult to recall which one and how many. This is some kind of an indication that no complications have ever occured in my practive with partial odontectmy. If there had been complications, I would certainly have remember…
Thank you for the question.
Best regards
Dr Sylvain Chamberland
Excellent article. Easy to follow with layman terms for everyone to understand. Answers all the questions I hear every day in the office.
Thank you Dr Webb for your kind words.
I wish you can use this article for your own patients. It is the intent of this website.
If you have any questions or suggestion of a case that could be discuss and helpful for layman, we can do it. Visit the french version of this site and you will see what I mean.
Best regards
Sylvain Chamberland