Hi Dr. Higgins,
Thank you for pointing out my error in the paragraph about Dr. Miller’s paper. I went back to the original paper and made the correction. I hope I got it right this time.
Xbow® and Forsus™
Maybe you can clarify if the mean treatment time of 24 months of the Xbow group included both phase 1 Xbow therapy and phase 2 with full edgewise brackets. Did the data of treatment time had a normal distribution?
Dr Proffit's lecture AAO 2017, San Diego
Since you attended Dr. Proffit’s lecture at the AAO meeting in San Diego, you certainly noted that he said that for clinical significance, one should
not only compare 2 means. The mean treatment time of the Xbow group was 24,18 ± 5,26 months and the mean for the Forsus group was 30,17 ± 7,66 months.
It would be interesting to divide the
treatment time in 3 groups:
<24 months,
24 to 30 months,
> 30 months, assess the number (or %) of patients Xbow and Forsus that were treated in less than 24, 24-30 or more than 30 months and find out if there is a
difference in the number of patients for each treatment protocol in
each strata of treatment time.
I think the
orthodontist clinician would benefit from knowing that using A or B protocol of treatment, chances are that Z% of the time the treatment time would be 24 months or less, Y% would be 24-30 months and so on…
That is how
Dr. Proffit told me to present the data on SARPE and the data of genioplasty. It gives a
much clearer picture of the outcome, especially when
the outcome data are not normally distributed, which
almost always is the case.
CAO 66th Annual Scientific Session, 2014
This webpage is a resume of the lecture I did at the panel on Fixed Appliance Management of Class II Malocclusion at the 66
th Annual Scientific Session of the Canadian Association of Orthodontist. The other panel members were Dr. Miller, Dr. Ramzi and Dr. Goodday.
I was the outlier who was not
promoting a Unitek product or a product in which I would have
financial interest.
My message was that
all these appliances work about the
same way.
Most studies showed:
- • Some restriction of Mx forward growth
- • No significant increase of Md growth
- • Significant dentoalveolar change at end of ortho
- • Class II correction is maintained at 2 y follow up (83%)
- • No significant skeletal change at 2 y follow up.
Among the side effect, incisor proclination occurred in spite of arch wire cinchback and -6° torque in the brackets. Therefore, wire-slot interplay should be reduced by using full dimensional arch wire and posterior cinchback. The use of TADs along with Class II correction device reduces lower incisors proclination (Aslan B, et al AO 2014;84;76-87). Extraction and cl II correction device is good marriage when space is necessary along cl II correction.
When comparing the
cost,
SUS2 was the least expensive followed by
Esprit corrector.
Forsus and
Twin Force Bite Corrector (TFBC) are about the same price, but more expensive than SUS2 and Esprit.
Xbow device was the
most expensive as one has to pay for the Forsus and the Xbow device. You will likely argue that if it saves some months of treatment, it may be worth paying extra dollars.
Nowadays, Carriere Motion appliance is gaining popularity. Dr. McNamara at the University of Michigan is conducting new studies with that appliance. The preliminary results are promising. The cost is about 270$ per unit so it ranks at the same price of Forsus and TFBC.
Carriere® Motion appliance permit the same advantage as Xbow reducing the treatment time of full fixed edgewise appliance. I am quite sure that side effect comes with the use of Carriere® Motion and this need to be managed.
Universal claims
Regarding the list of advantages to the Xbow appliance, many
apply to other class II corrector
devices :
1- Hyrax appliance can be use with any Class II corrector device, not only Xbow device.
3- If there is no buccal flaring, it is because there is a rigid trans-palatal device (an expansion device that is now not activated) maintain steady the molars. Any expansion device with any class II corrector device will do the same.
4- Asymmetric class II or class II subdivision is often explained by asymmetric growth at the condyle, one side being more distal than the other or by more mesial position of maxillary teeth on one side. This implies more distalization on class II side in the maxilla or mesialization of the class II side in the mandible. How can this can be achieve with the hyrax and the labiolingual appliance in place?
5- The need for phase 2. It is unlikely that despite adequate class II correction, there would not be other problems that need correction, like deep overbite, some rotation, some crowding. Therefore it depends on
how much compromise the patient or the orthodontist is willing to accept. I doubt that a phase 1 only Xbow case would routinely meet the standards for satisfactory treatment, much less pass the requirements of ABO case or Angle case.
6- The relationship of reduction of white spot lesion and Xbow is weak. White spot lesions are related to the maintenance of good oral hygiene whether the treatment is long or short.
7- Xbow opens space for the erupting maxillary canines. This is true for any device that would distalise maxillary teeth to gain space for the canine.
Regarding the relapse of side effect (item 2) that occur in phase 1 Xbow therapy, perhaps there should be
thanks to God that relapse exists. You don’t take cephs at the end of phase 1, but I often do. This permits to see the true effect of a given appliance. It is sad you did not.
Conclusion
I want to thank you for generating this discussion. I changed the paragraph to reflect Dr. Miller’s paper.
It gave me an opportunity to review cases that were treated with a labiolingual appliance.
In a private practice, I don’t have an ethics committee to tell me what to do, but keeping in mind the
ALARA principle, my
own ethics tells me to know what I have done with this or that appliance and that is why I may take a ceph after a particular phase of treatment. This is helpful to guide the mechanics of the phase 2.
In this sample of 3 selected cases, I can tell you that Phase 1 therapy with Labiolingual device (Xbow) and Forsus proclined the lower incisors by an
average 17° ((15+14+22)/3) which is about 3 times what is reported because they did not look at it. The side effects relapse 2° in one case, 15° in the other and a class I occlusion was achieved in both treated cases.
We can conclude that the Labiolingual appliance and Forsus device is effective to correct class II malocclusion, but
other class II corrector device can do the same. I think that Carriere Motion appliance is gaining in popularity and less Forsus device is employed nowadays.
Clinical case of Labiolingual appliance (Xbow)
I would like to share some cases with you and the public
Case 1


The picture on the left show the dental change following 5 months of Labiolingual appliance & Forsus device. Superposition of the tracing (pict on the right) shows proclination of the lower incisors of 22°, clockwise rotation of the occlusal plane and retraction of the maxillary teeth.
At the end of treatment, the red tracing show most side effect relapse and class I relationship was maintained.
The total treatment time was 23 months.
Case 2

.
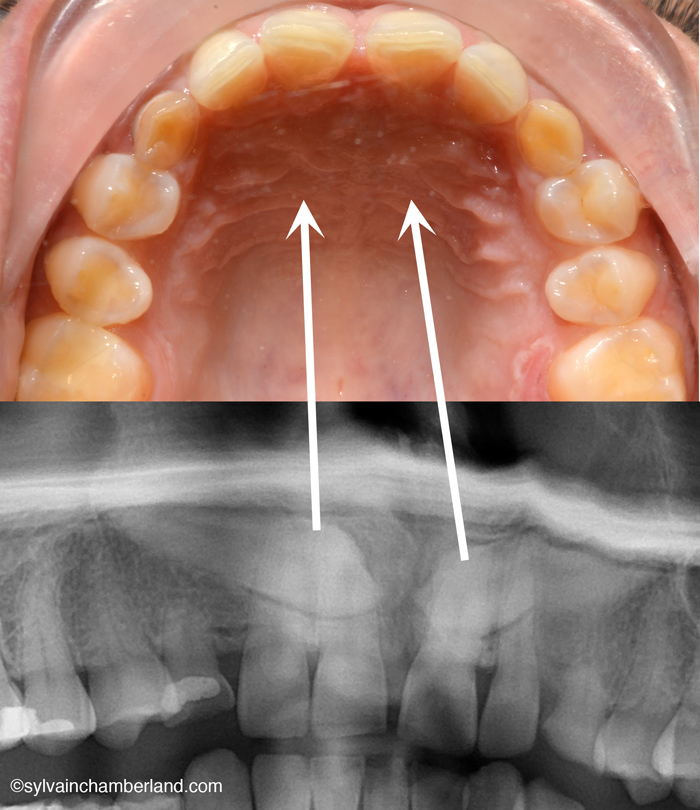
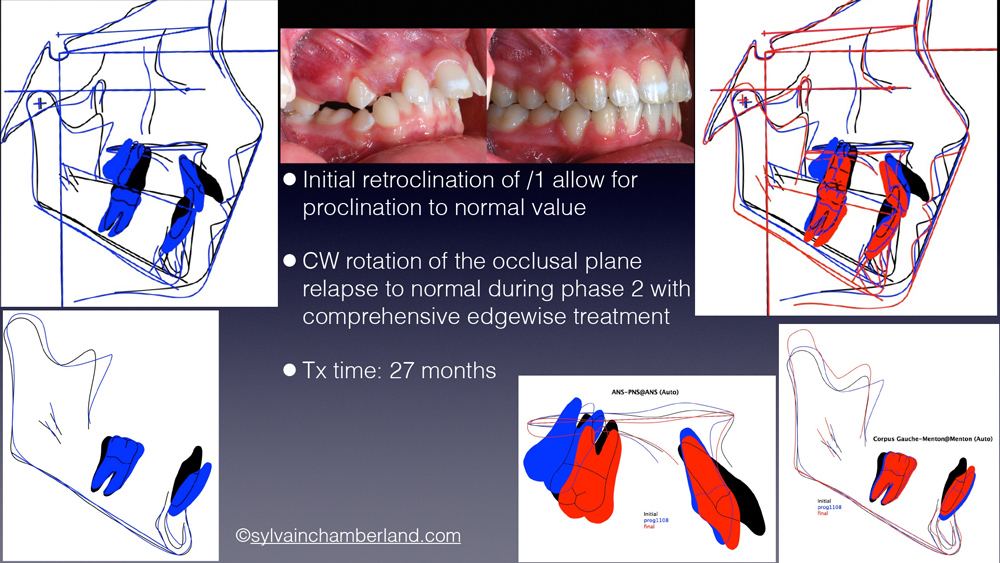
This 11 y. 5 m. old girl was in late mixed dentition, had retroclined lower incisors, impacted 23 and lip trap. The labiolingual appliance was selected because we could afford proclination of the lower incisors during phase 1 treatment. Lower incisors (/1-MP) was 93° at the end of treatment which is a normal value.
Case 3


.
This is a transfer case from a friend orthodontist in Toronto. Progress ceph was done at the removal of the Xbow device. The duration of phase 1 is 11 months. Like the other 2 cases, lower incisors proclined and the occlusal plane rotate clockwise.