Les commentaires
Dr Sylvain Chamberland, Orthodontiste dit :
Jennyfer,Est-ce que vous avez fumé après l'opération et durant la période de distraction?
Daniel dit :
orthochirurgie, Bonjour,Connaissez-vous un spécialiste en France ?
Je me pose en France à La rochelle, je suis en Nouvelle Calédonie pour deux mois encore et je vais m'installer ensuite à Mauritius.
Outre l'apnée du sommeil révélée récemment (31 épisodes/heure dont certain de 50 secondes), j'ai des endormissement diurnes de plus en plus fréquents.
Merci pour votre avis.
Dr Sylvain Chamberland, Orthodontiste dit :
Je ne connais aucun orthodontiste à Mauritius, ni à La Rochelle.Je suis désolé.
Je vous souhaite bonne chance dans vos démarches.
Dr Sylvain Chamberland, Orthodontiste dit :
Merci David for the clarification.Dr Sylvain Chamberland, Orthodontiste dit :
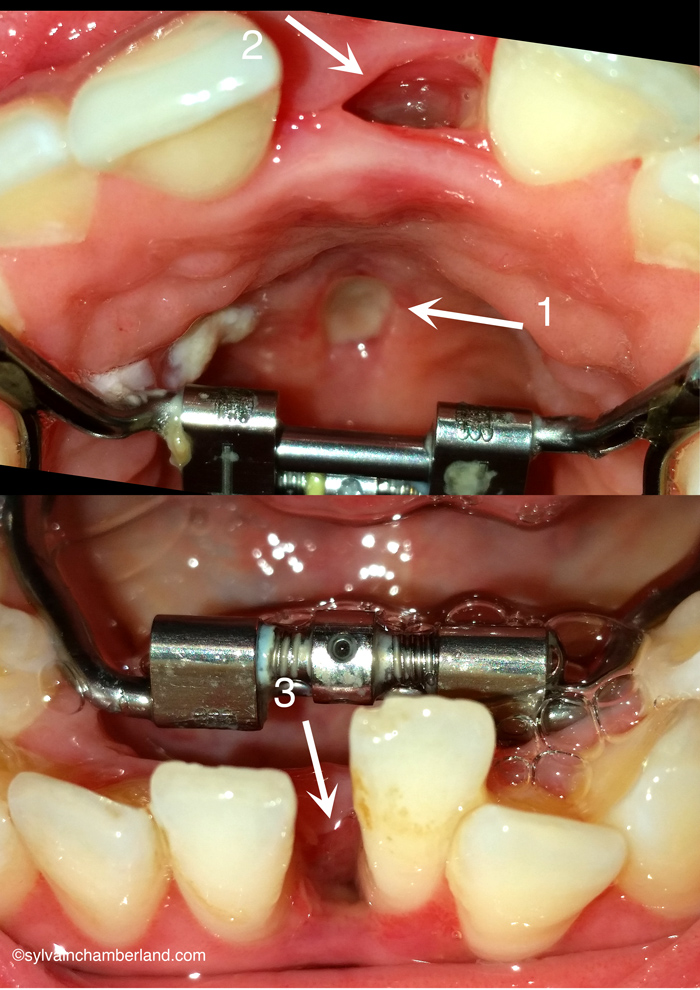 Fistule oro-nasale
Fistule oro-nasale
Wow!
Je fais de l'EPRAC depuis 1998 et de la distraction mandibulaire depuis 2001 et je n'avais encore jamais vu ce genre de complication bien que ce soit rapporté dans la littérature.
Au maxillaire, il s'agit bel et bien d'une fistule de la muqueuse palatine (flèche #1) qui communique vraisemblablement avec le trou près de l'incisive supérieure gauche indiquée par la flèche #2. La racine de la dent est exposée ce qui signifie qu'il y a eu fracture et possiblement perte du septum interdentaire.
Je crois qu'il y a eu trauma chirurgical lors de la manipulation de l'ostéotome et le septum a pu être fracturé et la muqueuse palatine lacérée.
À la mandibule, le trou indiqué par la flèche #3 démontre une exposition radiculaire compatible avec une perte du septum interdentaire. Je peux facilement imaginer qu'il y avait une proximité radiculaire des 2 incisives. Il aurait été plus prudent de faire la séparation entre l'incisive latérale et la canine. C'est la technique que nous privilégions dans les cas de proximité.
Je souhaite une bonne guérison, mais il y aura vraisemblablement des séquelles permanentes comme la perte de papille interdentaire et une récession gingivale.
Pour plus d'information, consulter le Keynote Distraction mandibulaire symphysaire et le clip de la chirurgie Mandibular symphyseal distraction.
Le cas qui est montré à la diapo #10 a eu une perte de septum sur l'incisive inférieure gauche. Cela ressemble à votre cas.
Je suis plutôt surpris que votre orthodontiste et votre chirurgien ait pris votre situation à la légère.
C'est certain que vous ne devez pas moucher votre nez tant que la fistule n'est pas guérie.
Dr. David Briss dit :
It was my pleasure to meet with Cary and go over his case.In my note I left out our discussion of the disc displacement; I did find anteromedial disc displacement with reduction, but with no limitation in any excursive movements, no history of pain or locking.
He did indicate to me that he has intermittent right ear pain, perhaps this is related to the more narrow nasal cavity on the right side, possibly some blockage resulting in intermittent middle ear inflammation.
Given the appearance of the condyles and the lack of a functional shift I doubt that the ear symptoms are related to the joint sounds.
Dr Sylvain Chamberland, Orthodontiste dit :
Thank you Dr. Briss for this thorough report. You were my eyes at far distance.Your tentative treatment plan is close to one of my hypotheses: extraction of 3 premolars and a sliding genioplasty. It is unfortunate that I missed the posterior right crossbite, but I could not see this from the reconstruction xray.
We went as far as we could get with an internet consultation.
I wish you all the best.
Dr David Briss dit :
I met Cary at my office yesterday, and on clinical exam he is Class II div 1 subdivision right malocclusion, maxillary midline deviated approximately 1mm left and mandibular midline deviated approximately 3mm right.There is slight bimaxillary crowding and an overbite of approximately 3mm. He has the remnant of a crossbite on the right side (1.6 and 4.6 are end-on transversely). Significant dental history is a PFM crown on 2.1, and he had orthodontics as a child, but no palate expansion was done. His chief complaint is facial asymmetry, particularly mandibular asymmetry and chin deviation.
The radiographic reconstructions he provided me seem to show the condyles positioned relatively well in the fossae. The cortex is intact, there is virtually no evidence of flattening of either condyle. There does not seem to be any evidence of pathology.
The panoramic reconstruction appears to show a deviation of the nasal septum to the right, but this is not obvious on the PA cephalogram reconstruction. In PA he does have a significant sloping of the floor of the nasal cavity, higher on the right than the left. The J points do not appear to be as asymmetric as the nasal floor finding might indicate. On facial examination his right orbit is noticeably higher than his left orbit. The chin is deviated to the right of the facial midline.
I suspect the etiology of his malocclusion and asymmetry is related to maxillary constriction, possibly a crossbite and mandibular functional shift that was never skeletally corrected during his prior orthodontic treatment.
In the absence of a current posterior or anterior open bite, and with images of well defined condyles I do not feel that there is either condylar hyperplasia on the left nor resorption on the right. It probably warrants followup at some time in the future, but at the moment it does not appear to be a progressive problem.
The only orthodontic treatment option that might satisfy his chief complaint would be combined orthodontics/orthognathic surgery. This most likely would be SARPE followed by limited orthodontics, then a Le Fort 1 for rotation of the maxilla (to the right) and asymmetrical BSSO with rotation to the left. However, this amount of treatment may result in only a small gain in aesthetics compared to a sliding genioplasty, and I would not recommend surgical orthodontics at this time. Additionally, an orthodontic-only treatment plan would perhaps correct the malocclusion to Class I bilaterally, but with no affect on the facial aesthetics, and is therefore not indicated either.
Dr David Briss
Orthodontist
5 Village Square
Chelmsford, MA 01824
Dr Sylvain Chamberland, Orthodontiste dit :
Vous pouvez vous procurer l'article au lien suivant: http://www.ncbi.nlm.nih.gov/pubmed/17636724Vous trouverez un lien pour l'achat du PDF chez Wiley online library http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003452.pub2/abstract
jennyfer dit :
Bonjour,Non il ne s'agit pas de l'espace entre les dents (ca je sais que c'est normal) mais belle est bien de la gencive, en gros ma gencive s'est "creusé".
Je vous envoie une photo sur votre courriel.
Dr Sylvain Chamberland, Orthodontiste dit :
Do you give the permission to publish a short report of your consultation with Dr David Briss?Dr Sylvain Chamberland, Orthodontiste dit :
Hi Cary, I have been informed that you visited Dr. David Briss. How was the consultation with him?Dr Sylvain Chamberland, Orthodontiste dit :
 Vous semblez décrire un espacement entre les dents qui se crée lors d'une procédure d'expansion. Si c'est ce que vous décrivez, alors c'est normal.
Vous semblez décrire un espacement entre les dents qui se crée lors d'une procédure d'expansion. Si c'est ce que vous décrivez, alors c'est normal.L'espace créé entre les 2 dents supérieures sera refermé orthodontiquement. L'espace créé entre la canine inférieure droite et l'incisive centrale gauche permettra l'ajout d'un implant pour les 2 incisives manquantes.
Dr Sylvain Chamberland, Orthodontiste dit :
Je ne comprends pas votre hésitation. Une canine incluse peut causer des dommages aux racines des dents voisines ou encore un kyste peut se former autour de la couronne.Votre question m'a rappelé le souvenir d'une question qui m'a été posée en 2013: Est-ce que je peux vivre sans canines?
Je vous recommande de lire cette page web où je révise les risques associés aux canines incluses.
Vous devez procéder à un traitement.
Cary dit :
Yes, you have my permission to publish anything related to my case. I only ask that sensitive information or anything among those lines be covered.Looking forward to seeing the story!
Cary dit :
And thanks again for all your help. Dr. Briss was great! Truly insightful. In the end, he felt my case wasn't severe enough to really consider jaw surgery, which I was actually happy to hear.Stephanie Mrad dit :
bonjour est-ce que vous pourriez m'envoyer tout l'article concernant le twin block publié dans Cochrane library que vous aviez mensionnéjennyfer dit :
Bonjour,Je faisais 2tours (2 1/4) en haut et 1 en bas et ce pendant 2semaines.
D'après mon chirurgien et 2 orthodontistes que j'ai vu ces "trou" dans mes gencives sont normaux. Celui du haut ne fait pas tout l'espace entre les deux dents donc je suppose que quand les dents reprendrons leurs places il disparaîtra. Mais celui du bas c'est surement créé car à l'origine les 2 dents étaient "collé" l'une à l'autre (ce sont les fameuses dents décalés) et avec l'écart entre elles ont peut voir qu'elles sont déformés tellement elles étaient collé....Donc là je n'ai pas de gencive du tout !
Fisun dit :
Bonjour Dr.Sylvain ,J'ai une question qui concerne le cas de mon fils Michel de 14 ans et demi.
Notre orthodontiste nous propose de faire une désinclusion de 23. Mais on est pas encore sûr et on aimerait l'avis d'un autre dentiste pour accepter ou pas ce traitement.
Je voudrais avoir également votre opinion pour notre cas.
Comment je peux joindre la radiographie.
Merci.
Inna.