Regards to extraction, I said premolars which are about 7,5 mm wide, not molars that are 10-12 mm wide. I said only one premolar in the lower left quadrant which will allow midline correction, but minimal lower incisors retraction if there is some crowding, a little bit more retraction if there is no crowding. The less the lower incisors are retracted, the less the effect on lip support. Nevertheless, we are talking about 1-2 mm of lip retraction.
Regards to surgery, you may benefit from orthognathic surgery if you want to have a straighter profile or correct the vertical asymmetry in the frontal plane.
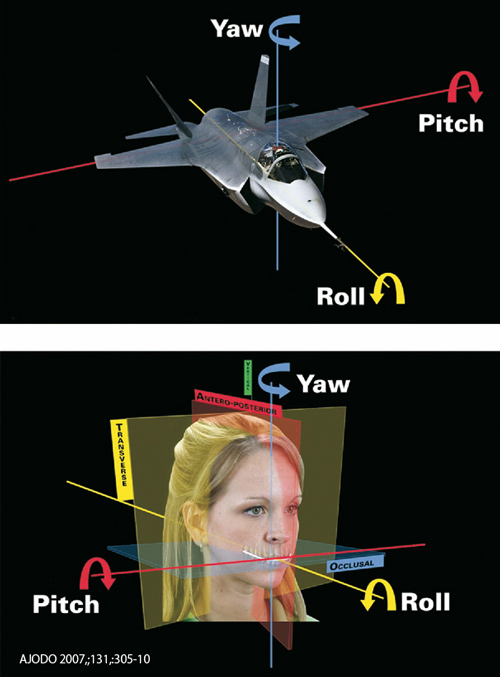
I am not sure you would need counterclockwise rotation of the occlusal plane (decrease pitch) because the 3D and ceph view shows a fairly normal angulation of the occlusal plane to the Frankfort plane (FH).
My concern is that you don't have an increase overjet, therefore, there is no room to advance the mandible. Extraction would be necessary to create an overjet that would allow mandibular advancement. If so, extraction of 1 lower left premolar may be what is needed (non-extraction in the maxillary arch).
Your facial asymmetry, if one wants to correct it, need "yaw" correction of the mandible and "roll" correction of both maxilla and mandible.

I did not have the profile view that would include your ear and your eye to correct and position it in the true horizontal relationship. With this profile view corrected to the plane "subnasale vertical" your mandible doesn't look that much retrusive.
Finally, I would like to clarify that if you elect to do an ortho treatment with or without surgery, the joint clicking may still remain. Orthodontic treatment of orthognatic surgery don't cure TMJ derangement.
The MRI will tell something about the disk relationship in the glenoid fossae. It does not say anything about growth activity. To assess growth activity, you need to have a bone scan (scintigraphy with Tc99).